 Therapeutic
Intranasal Drug Delivery
Therapeutic
Intranasal Drug DeliverySEDATION: Intranasal sedatives
Table of contents:
Introduction to IN medications for sedation (click here)
Literature review and discussion
Dental procedural sedation (click here)
Pre-operative sedation (click here)
Radiologic procedural sedation (click here)
Agitated adults - sedation with intranasal haloperidol, midazolam or lorazepam (click here)
Special Focus - Intranasal Ketamine for sedation
Intranasal flumazenil and intranasal naloxone as a reversal agents (click here)
Personal insights from experienced clinicians (click here)
Treatment protocol (click here)
Introduction
Interactions with medical providers are stressful experiences for children. Because of this stress and the anxiety it provokes, minor procedures often require mild to moderate sedation. Oral or rectal medications may be adequate for this sedation, however these delivery routes requires a considerable amount of time to take effect leading to delays in care and interrupted patient flow. Furthermore, since sedatives have wide inter-individual variations to response, it is difficult to find a single weight-based dose that is adequate to routinely sedate a patient but not so high as to cause prolonged sedation. This is not a problem if the medication can be titrated, but oral and rectal medications are not really reasonable methods for titration. Intramuscular injections suffer similar problems in terms of delay in effect (not as much as oral) and difficulty in titrating to adequate but not excessive sedation. A further major problem with IM injections is that they are painful and frightening to the patient. Intravenous therapy is the gold-standard for sedation – allowing rapid onset with titratable effect. It is ideal for any major procedure, but establishing an IV in a child is time and resource consuming for minor procedures. It also leads to an increased risk of respiratory depression due to the very high levels of medication that are achieved with bolus injection therapy. Finally, starting an IV is painful and frightening for many patients.
Intranasal and oral transmucosal (buccal, sublingual) delivery of sedative medications offers an alternative that provides some advantages over the above methods in properly selected minor procedure: they are faster than oral or rectal forms and less painful than injectable forms. Situations where investigators have found them to be useful include dental procedures, minor pediatric laceration repairs, anxiolysis prior to radiologic procedures such as MRI, pediatric preoperative sedation to assist with separation anxiety as well as sedation before other minor procedures including IV starts, biopsies, esophagogastroduodenoscopy (EGD) and ophthalmologic procedures.
The appropriate method and medication chosen for
sedation will depend on the clinical situation. If time is not an issue,
oral forms are adequate. If deep sedation and rapid titration are
needed, IV forms are probably indicated.
If mild to moderate sedation in a timely fashion is needed nasal
medications may be ideal.
The three most commonly studied medications for intranasal sedation are
midazolam, sufentanil and ketamine.
The following discussion will provide some insight into the
literature on this topic.
Literature overview and discussion
Dental procedural sedation:
The dental literature contains the largest
collection of data regarding intranasal medication use for sedation. In
one of the original articles on the topic, Abrams et al compared the
effects of single therapy with intranasal ketamine (3 mg/kg), midazolam
(0.4 mg/kg) or sufentanil (1.0 and 1.5 mcg/kg) in children getting brief
dental procedures.[1]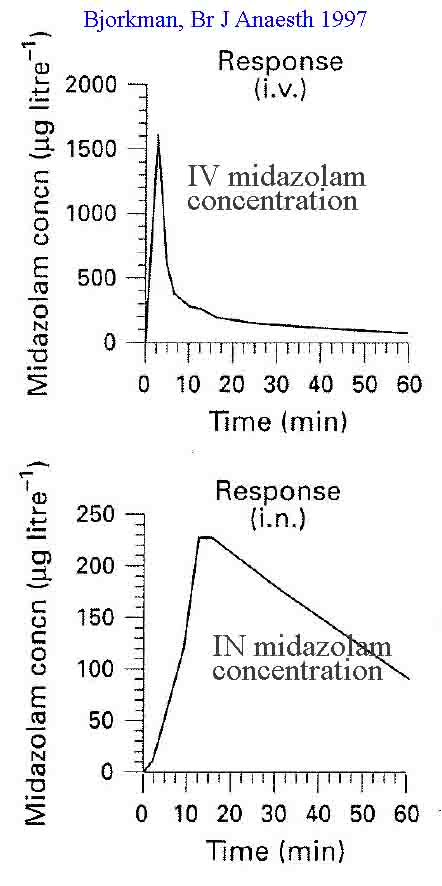 They felt either midazolam or ketamine worked
quite well (4/5 sedation score), as did the lower dose of sufentanil.
However, sufentanil at 1.5 mcg/kg led to over sedation and oxygen
desaturation. Ten years
later Roelofse et al compared combination therapy with intranasal
sufentanil plus midazolam (1 mcg/kg plus 0.3 mg/kg) versus intranasal
ketamine plus midazolam (5 mg/kg plus 0.3 mg/kg) 20 minutes prior to
induction in a dental surgery center.[2] They found both methods easy,
effective, safe and rapid in onset.
A smooth mask induction occurred in the majority of patients.
They concluded that intranasal medication is a promising method of
sedating preschool dental patients.
They felt either midazolam or ketamine worked
quite well (4/5 sedation score), as did the lower dose of sufentanil.
However, sufentanil at 1.5 mcg/kg led to over sedation and oxygen
desaturation. Ten years
later Roelofse et al compared combination therapy with intranasal
sufentanil plus midazolam (1 mcg/kg plus 0.3 mg/kg) versus intranasal
ketamine plus midazolam (5 mg/kg plus 0.3 mg/kg) 20 minutes prior to
induction in a dental surgery center.[2] They found both methods easy,
effective, safe and rapid in onset.
A smooth mask induction occurred in the majority of patients.
They concluded that intranasal medication is a promising method of
sedating preschool dental patients.
Another interesting finding is that compliance with nasal sedation is easier to achieve that with oral sedation in young children. Primosch et al found intranasal midazolam a useful alternative to oral midazolam in their dental clinic since a significant number of children (45%) refused to swallow the oral formulation.[5]
Ozen and colleagues compared nasal to oral midazolam in combination with nitrous oxide and found that the nasal formulation was superior in terms of successful sedation for the procedure.[71]
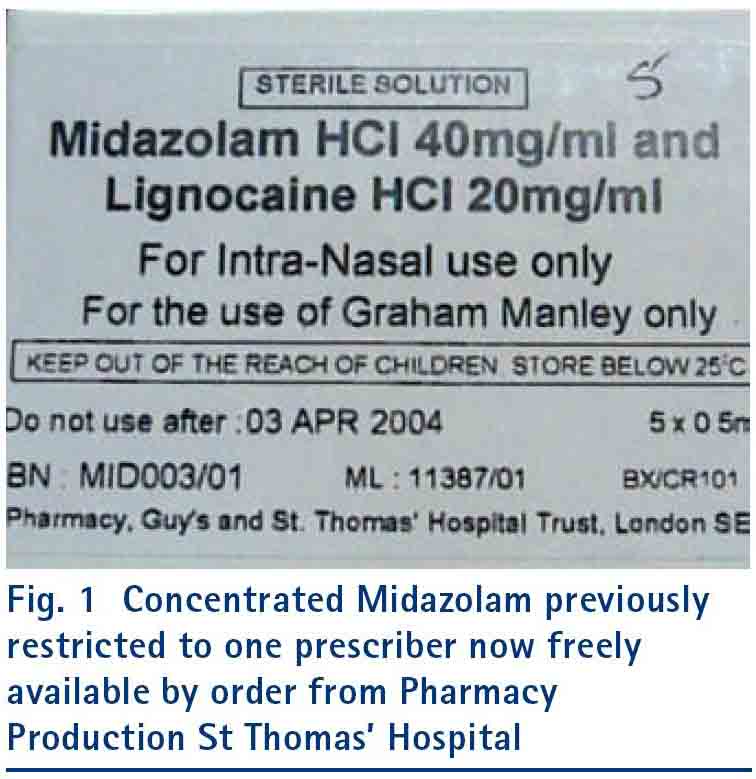
Manley et al describe their experience using intranasal midazolam to sedate adults with learning disabilities.[54] Due to dose-volume issues they concentrated the midazolam to 40 mg/ml (see photo below). They also added lidocaine to the medication to reduce burning during administration. They delivered 10 mg (0.25 ml) intranasally using a mucosal atomization device to enhance mucosal coverage. In a study of 222 adult sedations they found 93% success at sedation with no respiratory complications, allowing them to avoid the need for general anesthesia in the majority of cases. (Click here for article)
Manley 2008 - label for their concentrated midazolam:
In a follow-up prospective multicenter trial, Ransford, Manley and colleagues confirmed the efficacy of intranasal midazolam for sedation of adult dental patients with disabilities. They studied an additional 316 patients and found a dose of 10 mg of intranasal midazolam (the dose given to over 90% of cases) to be effective at sedation in 80% of adults, allowing IV cannulation and dental examination as needed. They noted a 3% incidence of oxygen desaturation that was easily reversed with stimulation and oxygen.[58]
Hitt et al investigated a combination of IN
dexmedetomidine ( 2 mcg/kg) plus IN sufentanil (1 mcg/kg) for use as a
moderate sedation regimen in children (3-7 years) undergoing dental
procedures. They used this combination in 20 patients and using an
independent observer as well and dentist and parental assessments found
it both effective and tolerable with 100% of procedures well tolerated
and completed safely.
Musani found intranasal midazolam to have more rapid onset and quicker
recovery than oral midazolam for preoperative sedation of children
undergoing dental surgery.
Peerbay compared IN midazolam at doses of 0.3 versus 0.5 mg/kg
to determine efficacy for sedating children prior to emergency dental
work.[138] They pretreated children with topical lidocaine a few minutes
before the midazolam and reduced burning sensation to only 9% of cases.
They found both doses led to sedation 100% of the time and both were
safe, however the 0.5 mg/kg dose resulted in more effective procedural
sedation.
Many other authors have used IN midazolam and or dexmedetomidine for pediatric and mentally disabled adult sedation and anxiolysis prior to procedures with generally good results and little if any safety concerns in doses ranging from 0.2 to 0.5 mg/kg. [6-13, 57,123,126,136,140,149,154,180,181]
Furthermore, many authors have now published extensive data using dexmedetomidine for dental procedural sedation. The overall impression is that this sedation is superior in length and depth of sedation making the procedure easier. This is likely due to the short duration and minimal sedation (more like anxiolysis) achieved with midazolam and the still prevalent problem of fear of midazolam and under dosing when it is used.[182-185]
In addition to these articles there is a discussion related to intranasal ketamine and dexmedetomidine for sedation (including dental patients) below.
The sum of this dental literature suggests that intranasal medications, specifically midazolam and dexmedetomidine, are easy to use and effective mild sedatives prior to dental procedures. The emerging data suggests that dexmedetomidine at 2-3 ug/kg is probably more reliable, though slower in onset and lasting longer. They can be used in non-compliant patients such as small children and mentally disabled adults and they have few significant safety issues reported.
Emergency department
and outpatient clinic procedural sedation:
A number of studies exist investigating intranasal medication delivery for minor procedural sedation in the emergency department. Acworth compared intranasal midazolam (0.4 mg/kg) to IV ketamine (1 mg/kg) plus IV midazolam (0.1 mg/kg) for minor procedural sedation in the emergency department.[14] Not surprisingly the IV therapy was more effective and easier to titrate – 100%. However, intranasal midazolam provided adequate sedation in 92% of patients and resulted in discharge 19 minutes earlier than the IV therapy group. The authors conclude that IV therapy is superior but that IN therapy may still be adequate in many minor procedures.
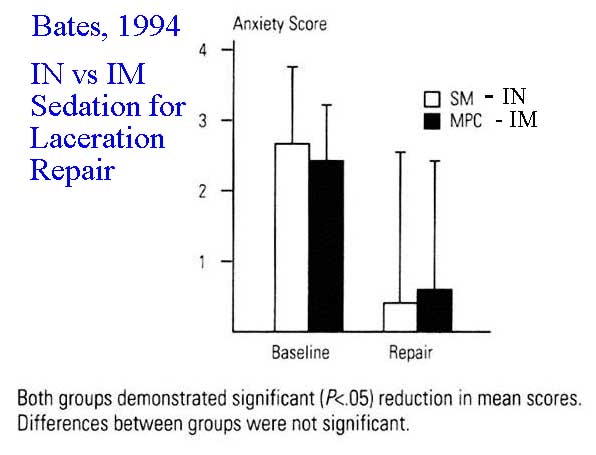
Bates et al investigated the combination of intranasal sufentanil (0.75 mcg/kg) plus intranasal midazolam (0.2 mg/kg) to an intramuscular injection of meperidine, promethazine and chlorpromazine (IM-MPC) for sedation prior to laceration repair.[15] The investigators chose these lower intranasal doses based on safety concerns with combined therapy. Based on past experience, they felt that these low doses of intranasal sufentanil or midazolam were not reliably effective if given as single drugs. Never the less, their results indicate that the combination of IN sufentanil and midazolam in low doses was as effective as intramuscular MPC in sedating children for laceration repair. Furthermore, since the children tolerated the IN medication better than the IM medication and they had both shorter recovery times and times to discharge it might be a preferred sedation method for minor laceration repairs.
Yealy et al report their experience with IN midazolam dosing in 40 children undergoing laceration repair.[16] They found that IN doses of 0.2 to 0.29 mg/kg were inadequate (27% adequate sedation), 0.3 to 0.39 mg/kg was better (80% adequate sedation) but 0.4 to 0.5 mg was best (100% adequate sedation). Onset of sedation averaged 12 ± 4 minutes, recovery 41± 9 minutes and discharge 56 ± 11 minutes. They do not report problems with desaturation or respiratory depression even at the higher dose. Theroux et al found similar efficacy of IN midazolam in doses of 0.4 mg/kg with marked improvement in patient cooperation compared to placebo.[17]
Klein conducted a well designed randomized controlled trials noting more rapid onset of action and superior sedation when midazolam was given intranasally versus buccally or orally.[63] As noted in almost all studies, the intranasal route burned with administration and caused more discomfort. However, as has been noted by other authors this burning is easily overcome by pretreatment with topical lidocaine (see discussion of concerning an article by Chiaretti reviewed in the next paragraph.)
Mellion et al conducted a study regarding onset of action and time of sedation for kids getting nasal midazolam for laceration repair.[167] They noted the drug peak was at about 10 minutes and effective sedation times lasted out to around 30 minutes with the best sedation in the 5-17 minute time range. This is important to understand so you are ready to begin the procedure shortly after drug delivery and optimize the use of the maximal sedation time. Here is the synopsis of their recommendations: Give the kid a nasal dose of lidocaine first then get all your tools out and ready (our recommendation); administer a weight based dose of nasal midazolam in the 0.4 to 0.5 mg/kg range (higher is better); as soon as they are goofy (about 5 minutes) position them, anesthetize and begin cleansing the wound (this requires some restraint as they are not unconscious); sew it. Do all this in 20-30 minutes if possible. If you will need longer sedation time for a complex wound consider alternate sedative like IM ketamine.
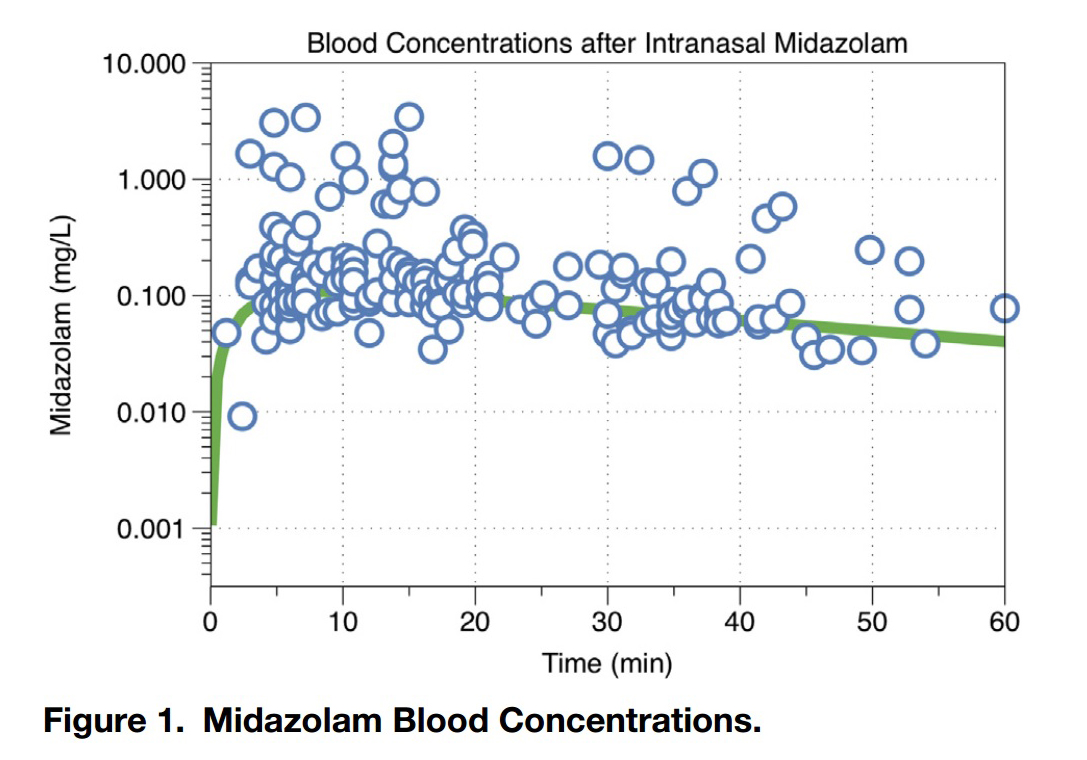
Mellion et al- Midazolam blood
concentrations: This graph demonstrates the rapid
absorption of 5 mg/ml generic midazolam when administered by a syringe
driven atomizer. The peak is in 10 minutes and the 90% of peak time
range is 5 to 17 minutes at which point it begins to drop off (this
is a logarithmic scale so the slope is not as steep looking as a
normal scale). This timing of the peak suggests the ideal time to do the
procedure (start work as soon as they are goofy which is about 5
minutes, go fast as it wears o ff relatively quickly).
Kawanda conducted a study using nasally delivered midazolam to assist with outpatient surgical interventions in a very poor area of Africa, where no anesthetists and very limited medical resources were available.[68] Here is the ultimate indication for nasal drugs - to cut costs and improve patient care even in a country with very limited medical resources. These authors were able to more comfortably perform procedures such as I&D abscesses, reduce femur fractures, do circumcisions, and perform thoracentesis using nasal midazolam. They found this therapy resulted in less crying, better cooperation, and they needed fewer assistants to restrain the patient. Their overall cost for care - atomizer device plus generic drug - was 4.5 Euros. They conclude "Intranasal midazolam is a cheap and effective way to treat pain in children during surgical procedures in poor countries, when anesthetists are not available, as well as making the surgeons job easier." My only suggestion is to add a nasal opiate to the mix to get both sedation and excellent pain control.
Acker and Jamieson investigated IN midazolam for a
minor pediatric gynecologic procedure – separation of labial
adhesions.[96] Here is their abstract:
“Use
of orally administered flavored midazolam elixir in the office setting
has been previously described as an
alternative to general anesthetic
for manual separation of severe or persistent labial adhesions. We share
the technique of using atomized intranasal midazolam for sedation (and
amnesia) that has quicker onset, shorter duration, and well described
safety and patient tolerance. This technique eliminates the problems
associated with a child who refuses to swallow the elixir.”
Shavit et al looked at another minor procedure that
is frequently performed – catheter urine collection from small girls at
risk for UTI.[97] They compared 163 sedated with midazolam (either oral
or nasal) to 174 who were
not. They found half as many contaminated specimens resulted (12% vs
26%) with no serious side effects and a slightly longer length of stay
in the ED (3 hours vs. 2.5 hours).
Shrestha
present an interesting use of IN midazolam in an ICU setting. They
report using midazolam to sedate a patient who pulled their central
line. Following this sedation they were able to re-establish central IV
access.
Neville et al conducted a RCT comparing IN midazolam to IN dexmedetomidine for emergency department laceration repair.[137] They found dexmedetomidine resulted in less anxiety than cases given midazolam suggesting this may be a superior drug choice for these procedures.
Cozzi reports two cases where low dose IN dexmedetomidine was useful for calming pediatric patients in acute respiratory distress (severe asthma) so they could be successfully treated and have IV established as their airway issues start to improve. This case presentation provides an interesting hypothesis for safely calming these high risk patients that deserves further investigation.[164]
Spalink also published an interesting case series demonstrating that nasal dexmedetomidine, an alpha 2 antagonist, was effective in acutely treating adrenergic crisis in 3 cases of familial dysatonomia.[170]
Nemeth et al published one of the few nasal drug delivery papers coming out of Germany. As these authors elude, German physicians have been a bit hesitant to adopt this treatment modality until they see more evidence from their own colleagues. Here is a very well done study using adequate doses of IN drugs and an atomizer to deliver the drugs – so the results should be reliable and believable. The authors provide good evidence that IN drug delivery is safe and effective for sedation and pain control when delivered by German clinicians to their patients using the protocols and doses they recommend.[171]
Ryan et al found that combining intranasal Fentanyl 2 mug/kg with midazolam
0.2 mg/kg they were able to reliably sedate 97.6% of pediatric ER
patients (n=546) requiring laceration repair with no events of hypoxia
or hypotension.
These findings were confirmed by Williams et al in the urgent care
setting where they also found midazolam and fentanyl (alone or in
combination) were effective and safe with no hypoxic events.
Guthrie et al did a chart review to evaluate their staff impression and
patient outcomes when IN ketamine was used for analgesia or mild
anxiolysis/sedation. They found high provider satisfaction and a drop in
use of IV medications for analgesia and sedation. Interestingly (but not
suprising if you have been paying attention for the last decade and are
willing to use the proper does to obtain you clinical effect) the
doctors prefered ketamine in the 3-5 mg/kg dose – higher than we see in
many studies. Side effects occurred in 6% but were all minor (nausea,
dizziness, drowsiness).
Concern occasionally arises regarding the NPO status of a child and the
safety of IN medications. Malia et al authors
looked into this in ED patients undergoing sedation with IN midazolam.
They found that 2/3 of patients had eaten within the last 2 hours
yet no patient in their study (112 patients) suffered from aspiration.
Comments: Emergency room procedures
frequently occur in suboptimal conditions and NPO status is usually
unknown or the patient has recently eaten or consumed liquids. Never the
less, the IN sedation literature demonstrates some nausea and vomiting
associated with dexmedetomidine (<1% generally) but
has no reports of aspiration to
my knowledge. This is likely due to the fact that IN medications do not
cause general anesthesia or even deep sedation – they generally put the
patient into a calm or sleepy state but they are easily aroused (as was
the case in this paper). In
this condition the patient can protect their airway so NPO status is not
really relevant. If you
really want “un" -conscious sedation then you should put in an IV, have
suction equipment available, get them on monitors and put them down.
Intranasal medications are the wrong tools for this type of sedation.
Miguez found that Orthopedic procedural sedation using IN fentanyl and
nitrous oxide was equally effective as IV ketamine with fewer side
effects and shorter lengths of stay.
Williams and colleagues reviewed their experience in a pediatric urgent
care and found that intranasal fentanyl and midazolam are safe and
effective in this less resource intense setting.
In summary, the majority of emergency department
sedation articles involve sedation prior to minor laceration repair in
children. Drug doses
required for successful sedation for laceration repair (midazolam at 0.4
to 0.5 mg/kg) need to be slightly higher than that described in the
dental literature where inhaled nitric oxides is often used in
combination. Combined nasal sufentanil plus midazolam or fentanyl plus
midazolam seems to be more successful
using lower doses of midazolam.
Dexmedetomidine in the ER is just showing up, and combinations of drugs
with ketamine is also starting to be investigated as ketamine alone via
the nasal route does not seem to provide adequate sedation though it is
an excellent analgesic.
Intravenous therapy is superior to intranasal therapy but requires an IV
to be established – a painful and resource consuming procedure.
In addition to these articles there is a discussion related to intranasal ketamine for sedation (including emergency patients) below.
Nasal burning with intranasal midazolam
One common symptom associated with IN midazolam is nasal burning for the first 30-60 seconds.[18] Bates did not find this to be the case with combined IN sufentanil and midazolam, whereas other investigators such as Everitt have found burning to be an issue when midazolam is used alone.[15, 18] The authors of this site have found this to be very common with midazolam but not with any other drugs. Parents should likely be informed of this initial side effect so they are not surprised if their child cries even with a nasal medication. Another option is to delivery topical lidocaine a few minutes prior to application of the midazolam. Chiaretti et al investigated this concept in a prospective clinical trial of 46 young children published in October 2010. After topical lidocaine sprayed (given by their mothers), all children received 0.5 mg/kg of intranasal midazolam – half the dose up each nostril. No child reported any nasal burning or bitter taste.[61] All children achieved the minimal goal of minor sedation (awake but sedated) and mild reactivity (mild reactions that do not disturb the procedure). Mean duration of sedation was 23 minutes – onset in about 7 minutes, off by 30 minutes. Doctor and parent satisfaction scores were very high (8.8 and 9.8 on a scale of 10). The sedation protocol was particularly helpful for peripheral IV placement. There were no serious side effects, no over sedation and no oxygen desaturation less than 95%. Manley [54], Ransford [58] and Antonio [70] all support the concept of combining lidocaine either before or at the same time as topical nasal irritant like midazolam to prevent burning and irritation.
Besides pointing out a new way to eliminate the burning seen with midazolam, Chiaretti's study also reaffirms how safe midazolam is when given via the nose. No reports exist of any significant respiratory depression or desaturation when IN midazolam has been used alone. This is likely due to the fact that intranasal midazolam delivery leads to drug absorption over a few minutes rather than an instant bolus that is seen with IV therapy. This slower onset of action probably prevents serum levels from crossing the respiratory depression threshold.
Peerbay compared IN midazolam at
doses of 0.3 versus 0.5 mg/kg to determine efficacy for sedating
children prior to emergency dental work.[138] They pretreated children
with topical lidocaine a few minutes before the midazolam and reduced
burning sensation to only 9% of cases.
They found both doses led to sedation 100% of the time and
both were safe, however the 0.5 mg/kg dose resulted in more effective
procedural sedation.
Smith et al conducted a double blind RCT comparing IN lidocaine to IN
saline pretreatment to determine if either reduced the pain experienced
when children are then administered nasal midazolam.[141]
This study is the most rigorous yet. The bottom
line – pre-treatment with 4% lidocaine markedly reduces discomfort
(nasal burning) experienced by children who are treated with nasal
midazolam. If you have not done so already here is additional evidence
supplementing many other articles on this web site suggesting
pre-treatment with lidocaine should be added to your IN midazolam
protocol.
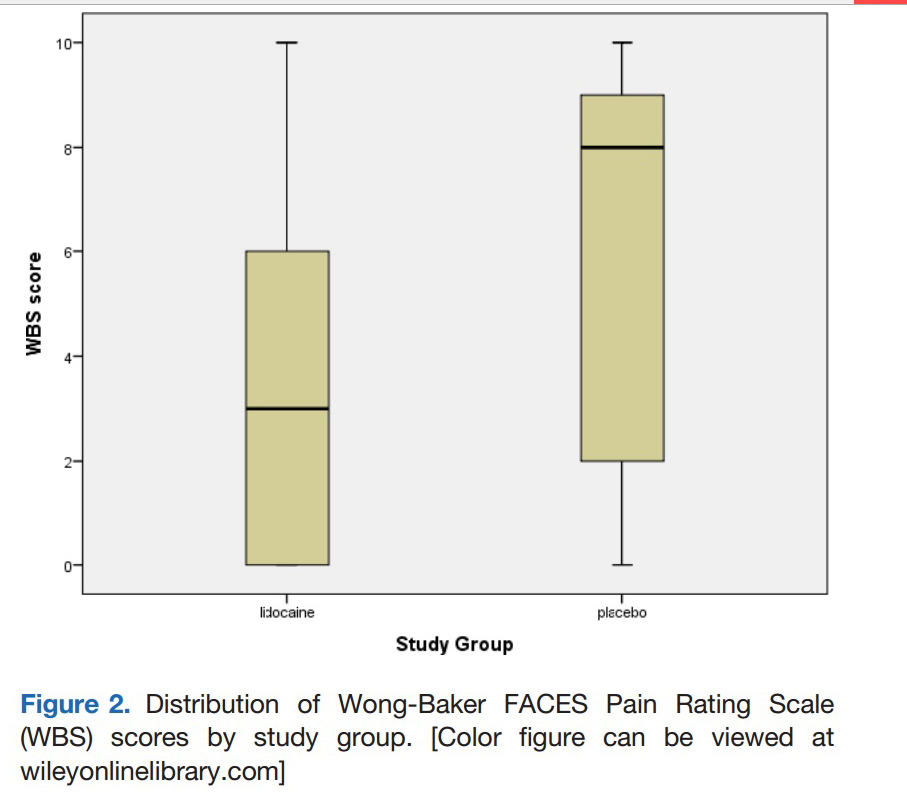
Smith et al: Graph contrasting pain scores of patients who received
lidocaine (WBS = 3) versus placebo (WBS = 8) 5 minutes prior to IN
midazolam administration.
Khalil published a study in 2019 reconfirming that pretreatment with
lidocaine dramatically reduces pain and increases parental acceptance of
intranasal midazolam. Median pain scores without lidocaine were 8/10 whereas
they were 1/10 with lidocaine.
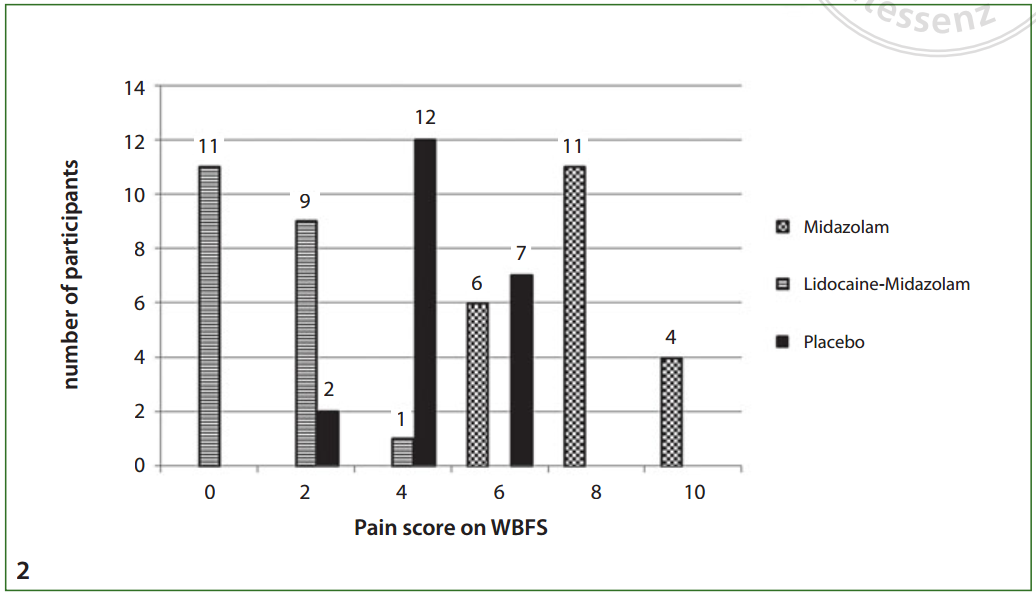
Khalil et al graph showing pain scores with and without pretreatment with lidocaine
Comment: Despite
10-15 years of literature on this issue – all referenced in these web
pages - many clinician still don’t pretreat with lidocaine. I don’t get
it. Its simple, effective, improves satisfaction and reduces stress for
everyone involved. I will continue to point out these articles until it
becomes standard care to include lidocaine on every nasal midazolam
sedation case. Just do it.
Pre-operative sedation:
Separation anxiety and acceptance of the mask during induction of general anesthesia are issues that lead many clinicians to prefer sedating children in the pre-operative phase before they take them from their parents into the operating theatre. Oral medications are commonly used but have considerable delays in onset, whereas IV and IM medications are painful and frightening. This has led several investigators to consider intranasal medications as an alternate method of achieving smoother separation and mask acceptance.
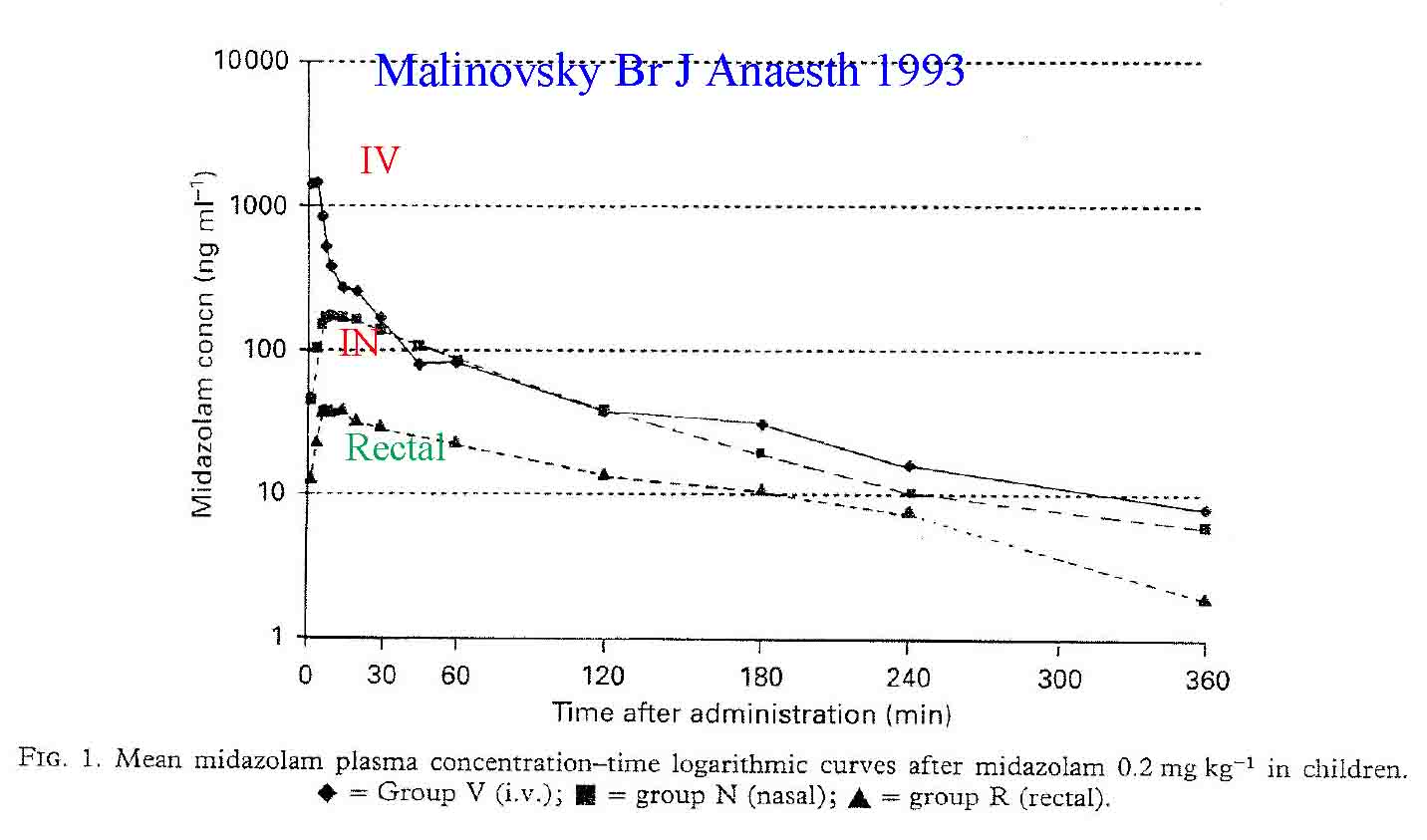
Malinovsky et al compared the time of sedation onset and peak serum midazolam levels in children randomized to intranasal (0.2 mg/kg), oral (0.5 mg/kg) or rectal (0.3 mg/kg) medication for pre-operative sedation.[19] They found the mean onset of sedation was fastest and peak levels highest for nasal midazolam (7.7 minutes, 146 ng/ml peak at 11.5 minutes) compared to oral (12.5 minutes, 104 ng/ml peak at 21 minutes) and rectal dosing (16.3 minutes, 93 ng/ml peak at 23 minutes). The authors conclude that intranasal midazolam is an excellent alternative for rapid premedication of pediatric surgical patients.
Bayrak et al investigated oral midazolam (0.5 mg/kg), oral tramadol (0.3 mg/kg) and intranasal sufentanil (2 mcg/kg) for pre-operative sedation.[20] They found oral midazolam and intranasal sufentanil very effective for sedation and mask acceptance. However, IN sufentanil at this high dose led to significant decreases in oxygen saturation and respiratory rate – an effect they accepted since they placed the patients under general anesthesia shortly thereafter. Karl et al conducted a similar study comparing low dose IN midazolam (0.2 mg/kg) to high dose intranasal sufentanil (2 mcg/kg).[21] Both drugs markedly reduced separation anxiety, however they also found this dose of sufentanil led to oxygen desaturation as well minor chest wall stiffness. Zedie also compared intranasal midazolam (0.2 mg/kg) to intranasal sufentanil (2 mcg/kg) and found both equally effective at sedation.[22] They noted more nasal irritation and crying with the midazolam (71% versus 20%), but more nausea and vomiting and perhaps slightly reduced respiratory compliance with the sufentanil (34% versus 6%). Both drugs resulted in easy separation of the children from their parents.
Weber et al found that adding intranasal ketamine to midazolam further enhances onset of action with slight improvement in sedation.[23, 24] Weksler et al studied intranasal ketamine alone (6 mg/kg) and found it superior to intramuscular meperidine and promethazine for sedating children.[25] Many additional authors have similar experiences with easy separation and acceptance of mask ventilation following pretreatment of pediatric patients with intranasal midazolam.[26-30] Other investigators confirm the efficacy of intranasal sedatives, though nasal burning with midazolam was commonly described.[31-33, 66]
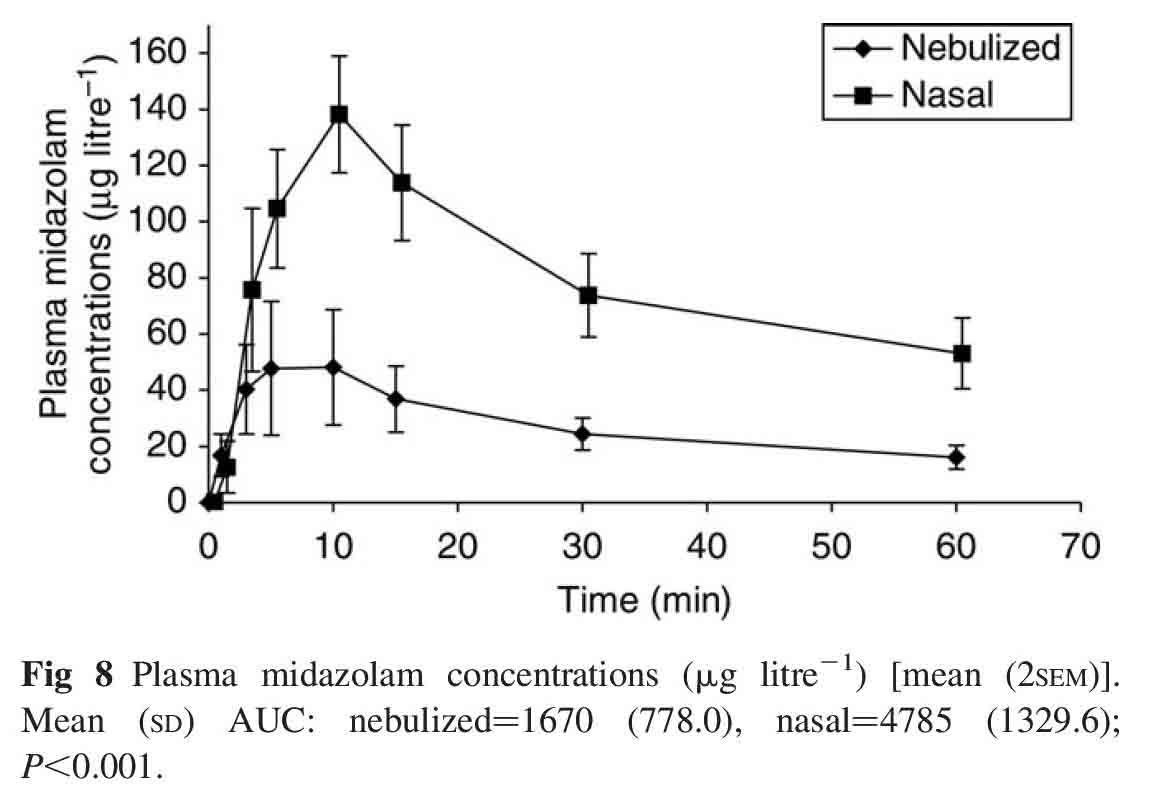
McCormick et al conducted a study with a bit of a twist - they investigate4d the efficacy of intranasal midazolam versus nebulized midazolam.[55] The nasal route resulted in far higher plasma levels, more sedation of faster onset. This is not surprising since many studies show that most nebulized drug ends up in the environment and not in the lung.
McCormick 2008: Plasma levels of midazolam following intranasal versus nebulized delivery:
Neonatologists have even found intranasal midazolam useful for sedation of the newborn. Baleine et al demonstrated that IN midazolam was an effective method to induce sedation prior to intubation in preterm neonates requiring emergent intubation despite no IV access. [102] Similarily Milesi et al investigated the efficacy of nasal midazolam (0.2 mg/kg) versus nasal ketamine ( 2 mg/kg) for sedating neonates who needed urgent intubation for tracheal suction.[168] They found nasal midazolam to be effective in 89% versus ketamine in only 58%. This should not surprise our readers as the data is very clear that nasal ketamine is very effective for pain control in this dose range, but a MUCH higher dose is needed for sedation. However, this study is important for another reason – it is one of our few studies noting both safety and efficacy of nasal drugs in neonates who often do not have IV access readily available.
Akcay et al report that a
Midazolam Ketamine combo (0.1 mg/kg and 3 mg/kg) was superior to either
alone for preoperative sedation, but their midazolam doses were
inadequate for sedation (0.2 mg/kg) and their ketamine doses barely hit
a level that has worked in the past (5 mg/kg)
Milesi et all found that intranasal midazolam was 89% effective at sedating premature neonates (average age 28 weeks gestation, average weight 1100 grams) for endotracheal intubation. IN ketamine was not as effective at sedation (58%). [175]
In addition to these articles there is a discussion related to intranasal ketamine for sedation (including pre-operative patients) below. Furthermore many additional abstracts exist but have not been discussed here due to their lack of new information. The sedation abstract section has many of them listed alphabetically by first author or you can just search Pubmed.
Intranasal Dexmedetomidine and clonidine for sedation:
Recent interest has emerged in the anesthesia literature regarding α2 adrenergic agonists for sedation. The two medications investigated are clonidine and dexmedetomidine. These drug act on the CNS in the area of the locus ceruleus and induce EEG activity that resembles natural sleep. Patients who are treated with intranasal alpha-2 agonists are easily aroused - perhaps due to the sleep like state they are in - but they are also not as "silly" as those given midazolam, nor do they obtain amnesia to the events. The potential advantages of these drugs over nasal midazolam appear to be due to the fact that no transient nasal burning occurs, reduced confusion state is present after the procedure and there is no respiratory depression risk from the medication.
Talon et al conducted a randomized, controlled trial on 100 children comparing intranasal dexmedetomidine (2 ug/kg) to oral cherry flavored midazolam syrup (0.5 mg/kg).[51] He found dexmedetomidine to be more effective at inducing sleep and equivalent to oral midazolam in terms of conditions at induction (45 min later) and emergence. They also felt nasal medication was easier to administer because the child could not resister or spit it out. They concluded that intranasal dexmedetomidine was rapidly effective, reliable, safe and relatively less traumatic than oral midazolam syrup for pre-operative sedation.
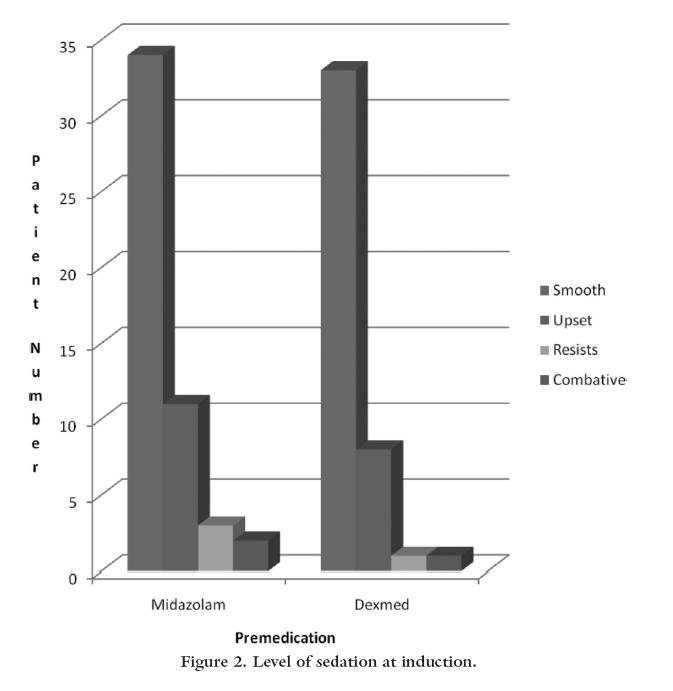
Talon et al - Level of sedation following intranasal dexmedetomidine versus oral midazolam
Yuen et al compared two different doses of intranasal dexmedetomidine (0.5 or 1.0 mcg/kg) to oral midazolam (5 mg/kg) in a preoperative sedation study of 96 children.[43] These authors found both doses of dexmedetomidine to be superior to oral midazolam for sedation and more adequate sedation at induction was present in patients receiving the 1.0 mcg/kg dose. In a follow-up study these authors found the onset of action of IN dexmedetomidine to be 25 minutes and duration of action to be 85 minutes.[59]
Stella and colleagues reported 3 cases of intranasal clonidine (1.5 to 2.0 mcg/kg) sedation in children.[44] In one case it was used to rescue a child who was having paradoxical agitation due to oral midazolam, another was a child who had many experiences with oral and nasal midazolam and refused any more - but was willing to try clonidine and did well with it. The third was a 3 month old agitated, hypertensive child with renal disease who obtained both sedation and blood pressure control with nasal clonidine. In all cases onset was within 5 minutes. Both groups of authors found these medications useful for selected patient populations and suggest further research be conducted.
Sakurai noted transmucosal buccal dexmedetomidine was safe and effective for preoperative sedation of children.[56] They also found that the sedation was deeper than that achieved with rectal diazepam. The effective dose they used was 3-4 mcg/kg - slightly higher than other authors possibly due to the somewhat less bioavailability typically seen with buccal compared to nasal drugs. Sayal and colleagues found a nasal dose of only 0.5 mg/kg was ass effective as a similar dose of nasal midazolam for preoperative sedation (abstract - click here).
Mukherjee
conducted a study comparing oral to nasal clonidine as a premedicant for
pediatric population.[60] Two dosage of clonidine were used by both
routes to determine optimum route and dosage of clonidine that produces
optimum effect, quick onset and without any significant side effects.
Sixty ASA grade I and II patients of either sex with age ranging between
1-7 years were scheduled for various elective surgical procedures of not
more than 90 minutes duration in randomized prospective manner. The mean
onset time for the intranasal group was 21.6±10.7 minutes (group 4 ug/kg)
and 29.8 ±9.5 min (group 3ug/kg) while for the oral group it was 40.3 ±
6.7 min (group 4 ug/kg) and 47.1 ± 7.1 min (group 3 ug/kg). Sedation was
mild but not deep – more of an anxiolytic than a deep sedative.
It was well tolerated by both routes. The authors conclude that
clonidine premedication causes
anxiolysis and sedation leading to good mask acceptance and smooth
induction. Nasal clonidine is felt to be better because of quicker onset
of action compared to oral clonidine. Therefore, intranasal clonidine at
a dose of 3 ug / kg-body
weight may be preferred as higher dose does not improve the quality of
sedation.
Other d
Sheta et al compared IN dexmedetomidine (1 mcg/kg) to midazolam (0.2
mg/kg). in children undergoing dental rehabilitation. Not surprisingly
given the doses that are know to be too low for midazolam, the midazolam
was not as effective and it caused nasal burning while the
dexmedetomidine, as predicted, took longer to work . [108]
Mitra et al randomized 60 children to either IN
midazolam 0.3 mg/kg (5 mg/ml generic solution) or IN clonidine 4 mcg/kg
(150 mcg/ml solution) plus 0.6 mg of atropine.[101] The primary outcome
was adequate sedation at 30 minutes. Secondary outcomes were crying
after drug delivery and mask acceptance in the operating suite. All 60
patients (30 per group) achieved adequate sedation by 30 minutes though
it was faster onset (20 minutes) with midazolam. The clonidine group had
better acceptance of the drug with less crying and they had better mask
acceptance and calmer awakening. The authors conclude: “intranasal
clonidine has been shown to produce comparable level of sedation as
effective anxiolysis as nasal midazolam after 30 min, but with a better
mask acceptance and recovery profile.”
Han et al compared IN to IV dexmedetomidine for sedation prior to
gastric endoscopy and conclude the IN route is superior due to more
stable effects on the respiratory and circulatory parameters with fewer
adverse reactions.
Patel et al provide a case report of syncope and bradycardia following
IN dexmedetomidine and cystourethrogram in an 11-year-old girl. They recommend monitoring in the setting of
dexmedetomidine induced sedation and point out this as a rare (single
report) possible complication.[113]
Cheung et al note that IN
dexmedetomidine “confers deeper perioperative clinical sedation with
significantly less use of additional sedatives during upper
gastrointestinal endoscopy” when compared to placebo plus patient
controlled anesthesia.
Mekitarian et al provide
further confirmation of the efficacy in IN dexmedetomidine for pediatric
MRI acquisition – noting sedation in 13 minutes and no failures or
significant adverse events.
Mukherjee et al conducted
an study in children investigating the incidence of emergency agitation
and sedation when children were given IN dexmedetomidine versus IN
clonidine. Intranasal dexmedetomidine 1 mug/kg was more effective than
clonidine 4 mug/kg in decreasing the incidence and severity of emergency
agitation, when administered 45 min before the induction of anesthesia
with sevoflurane for pediatric day care surgery. Dexmedetomidine also
significantly reduced fentanyl consumption in PACU. It did lead to more
prolonged sedation however.
Tang et al noted improved postoperative comfort and decreases stress
hormone and inflammatory mediator levels in patients given intranasal
dexmedetomidine prior to endoscopic sinus surgery (FESS).
Bhat el al compared IN dexmedetomidine (1 mcg/kg) to combined IN
dexmedetomidine plus ketamine (1 mcg/kg plus 2 mg/kg) for preoperative
sedation but found no differences in sedation and relatively poor mask
acceptance for either group.[143] This is not surprising as both drugs
are dosed at a fairly low dose and based on prior literature would not
be expected to be very effective.
Lu et al compared IN dexmedetomidine to IN placebo in 81 adults (NOT
children) to determine its efficacy for pre-operative sedation and
anxiolysis.[147] It worked well despite a fairly low dose (1 mcg/kg) and
did not lead to increased recovery times.
Li investigated the incidence of bradycardia in 9984 pediatric patients
receiving intranasal dexmedetomidine. 2.3% developed bradycardia but it
was never of clincal importance and did not require intervention.
This article is important due to the
slight concern surrounding dexmedetomidine induced bradycardia. This
article specifically investigated this issue in a very large patient
cohort (9984 uses). While they confirmed bradycardia in 2.3%, it was
never clinically important and easily resolved with patient stimulation.
In a larger study by Yang - below, 17948
patients were sedated with intranasal dexmedetomidine. They only
reported clinically significant cardiac effects – 1 child with PAT
developed PAT during the sedation, 4 children (0.02%) developed heart
rate/BP changes more than 20% outside the normal range. Both authors
conclude that adverse events and bradycardia are very rare.
Yang et al present data on over 17,000 children treated with
intranasal dexmedetomidine (2 mcg/kg plus IN ketamine (1 mg/kg) for
procedural sedation. They found it 93% effective with a median sedation
time of 62 minutes and recovery time of 45 minutes. There were very few
adverse events ( 3 airway events requiring emergent intervention in this
large group).
Li et al conducted a dose finding trial to determine the 95%
effective dose for pediatric sedation using IN dexmedetomidine.
They found that dose to be 2.64 mcg/kg. Using this dose sedation onset
was 15 minutes and wakeup
time was 40 minutes later.
Preoperative Sedation summary:
In summary, generic midazolam, sufentanil,
ketamine, clonidine and dexmedetomidine (which is not generic) all appear effective in sedating children, reducing separation
anxiety and improving mask acceptance in the pre-operative pediatric
setting. Midazolam can lead
to nasal burning and crying while sufentanil at high doses (2 mcg/kg)
can cause excessive respiratory depression and mild chest wall
stiffness. The α2 adrenergic agonists appear
to cause more of a sleep like state - easing separation, but also easily
aroused. The option of intranasal preoperative sedation might be most
useful in situations where the prior case ends quickly and the next
patients has not had sufficient time for their oral medication to take
effect (or has not even received it). In this case, nasal sedatives are
rapidly effective (5-10 minutes), reliable and possibly titratable.
Detailed document describing IN dexmedetomidine use for multiple sedation procedures
IN Precedex for CT scanning abstract
IN dexmedetomidine for preoperative sedation abstract
Radiologic
and cardiology procedural sedation (relief of claustrophobia,
anxiolysis for MRI, calm for echocardiography)
Sedation for radiologic procedures is commonly administered to prevent excessive patient motion and for problems with claustrophobia. Agents with rapid onset of action, short duration of effect and ease of administration are preferred for these relatively brief, painless procedures. Since intranasal medication delivery with midazolam fulfills all of these criteria it has been used in multiple studies with excellent results.
Low doses of intranasal medication (midazolam)
appears to be especially effective for cross-sectional imaging such as
MRI and CT. Hollenhorst randomized adult patients scheduled for MRI to a
single dose of 4 mg IN midazolam versus placebo.[34] They found they
achieved better quality exams with no cancellations in the study arm,
whereas the quality decreased and 15% could not complete the MRI in the
placebo group. Tschirch et al randomized adult patients to nasal (1-2 mg)
versus oral midazolam (7.5 mg). Patients treated with nasal midazolam
had a 97% success rate in obtaining a quality MRI while half of the
orally treated patients could not finish the exam.[35] These authors
view low dose IN midazolam as an effective and patient friendly solution
to overcoming anxiety and claustrophobia in patients undergoing MRI.
In a similar study Moss et al found they could reduce the need
for IV sedatives from 67% to 17% by using IN midazolam prior to MRI
imaging. Louon and Reddy also noted effective sedation and improved
computed tomographic image quality when using a combination of nasal
ketamine and midazolam in pediatric patients.[36] Weber compared IN
midazolam to rectal chloral hydrate prior to brain imaging.
Midazolam was effective in 82% of cases with mean time to test
completion being 55 minutes.
Chloral hydrate often required re-dosing to complete the study
(70% completed) and required 42 minutes additional time to successfully
obtain images. There was a clear preference of the nursing staff for
intranasal midazolam over rectal chloral hydrate. Harcke and Grissom
found 0.2 mg/kg of IN midazolam adequate to calm their pediatric
patients for imaging studies and recommend its routine use with pulse
oximetry as a safe and effective minor sedative.[37]
Chokshi et al. found atomized intranasal midazolam at a dose of 0.5mg/kg
very effective for separation anxiety
and sedation for both MRI and CT scans in children.[98]
A study by Filho et al
evaluated the utility of IN midazolam for sedation of children prior to
CT scanning.[100] They found it to be reliable, predictable, with little
side effects, allowing high quality CT
imaging with little artifact. The conclusion:
“this appears to be a useful technique of safe sedation for
imaging that could be valuable in pediatric emergency departments.”
Zhang et al found dose of intranasal dexmedetomidine
at 1 mcg/kg versus 2 mcg/kg adequate
for successful MRI acquisition in infants aged 1-6 months in
94% versus 98% of cases.
Tug et al found that intranasal dexmedetomidine at
doses of both 3 mcg/kg and 4 mcg.kg were effective for sedation of
children ages 1-10 years of age to obtain an MRI. The higher dose
resulted in better separation scores from parents.
Ghai et al found that IN
dexmedetomidine (2.5 mcg/kg) was far superior at sedation for CT
scanning than oral midazolam (0.5 mg/kg).
Gu found that the median effective dose of intranasal dexmedetomidine for children less than 3 years old who required sedation for a transthoracic echo was about 2.2 ug/kg.[197]
Yang determined the dose of intranasal dexmedetomidine that was effective
at least 50% of the time at sedating children for echocardiography. They
found it to be 2 ug/kg for children with acyanotic heart disease and 3.2
ug/kg for those with cyanotic heart disease.
Liu found that the dose of intranasal dexmedetomidine that was effective 90% in at least 90% of children less than 3 years old who required sedation for an EEG was 3.28 ug/kg.[198] In another study he found 96% successful sedation for TEE using 2 ug/kg of IN dexmedetomidine and 1 mg/kg of IN ketamine[199]
In 2019 Yang et al published a giant study reviewing the efficacy of IN
dexmedetomidine (2 ug/kg) plus IN ketamine (1 mg/kg) for procedural
sedation prior to radiology testing in children. They found the
combination to provide effective sedation in 93% of cases with onset of
action in 15 minutes and length of sedation about 1 hour.
This article is very useful due to its huge size and the
information we can glean from a single paper about efficacy and risks.
These authors used a combination
of medications and their procedures were primarily radiology based (not
painful, not stimulating to the patient) so their dose of
dexmedetomidine is probably right on at 2 ug/kg.
Prior studies have shown this to be the 50% effective dose for
stimulating procedures. Adding Ketamine probably helped a little to push
their efficacy up to 93%. Out of over 17 thousand cases they had 3 cases
that required airway interventions – all were known in advance to have
upper airway obstructive anatomy and so once sedated developed worsening
obstruction requiring intervention.
There were 4 minor events related to pulse or blood pressure for
which they intervened pharmacologically. Nausea and vomiting was the
most common adverse event occurring in 0.3% of patients, not resulting
in aspiration and easily controlled with ondansetron.
M
In addition to these articles there is a discussion related to intranasal ketamine for sedation (including radiology patients) below.
Second dose "titration" of intranasal midazolam
Lazol et al describe their experience using intranasal midazolam for minor sedation prior to pediatric echocardiography.[52] These authors review their results on 100 patients, using 0.2 to 0.3 mg/kg IN midazolam for the initial dose, and following up in 10-15 minutes with a second identical dose if inadequate sedation was present. They achieved 24% adequate sedation with the initial low dose, and 80% adequate sedation following the second dose. They report no adverse effects with either dose. This study points out a key component to sedation and pain control that most clinician are already aware of - the concept of titration to effect. Like IV medications, nasal sedatives and pain medications demonstrate inter-individual variation in patients, requiring additional dosing to achieve adequate effect. Fortunately, titration is possible and if one dose is not adequate, simply give another dose. A second observation can be made from this study - that of using an adequate initial intranasal dose in the first place. Many clinicians fail to use adequate IN drug doses, have inadequate effect and assume the drug is not useful when given via the nose - because they are u sing IV doses rather than the needed higher nasal doses. Based on extensive publication data and personal insights from years of use, the authors of this web site suggest an initial dose on 0.4 to 0.5 mg/kg of intranasal midazolam since lower doses are well known to be inadequate most of the time (the exception being if you simply wish the patient to be calm for a CT scan, but do not intend to do any procedure- in which case a lower dose such as in this study would be adequate).
In summary, nasal midazolam is very effective both in adults and children for sedation prior to CT and MRI imaging as well as for echocardiography. The use of this method speeds up patient care, reduces the rate of incomplete exams and improves the image quality. Fairly low doses (0.2 mg/kg in children, 1-4 mg total in adults) are effective and safe for CT and MRI, while higher doses appear to be warranted, and titration to effect is needed in invasive procedures such as echocardiography.
Miscellaneous sedation (ophthalmology, endoscopy, neonatal
sedation, biopsy)
Numerous additional indications have been described
for intranasal sedation including upper GI endoscopy, ophthalmologic
examinations in the anxious patient and minor biopsy procedures. Two
studies have found IN midazolam to provide acceptable amnesia and mild
sedation for EGD, though IV therapy was superior.[38, 39] Gan et al note
that patients who have failed chloral hydrate sedation can be “rescued”
and procedural care continued if IN dexmedetomidine is administered to
those who have failed. In their RCT
of 60 patients, a dose of 2 mcg/kg was far superior (93.3%
effective) to a dose of 1 mcg/kg (66.7% effective).[145]
Baier et al show that
using moderately high doses of dexmedetomidine initially (2.5- 3mcg/kg)
and allowing a second dose of 1 to 1.5 mcg/kg to be administered if
adequate sedation was not achieved they could successfully sedate 99.1%
to 100% of children undergoing electroencephalogram and auditory brain
response testing with minor side effects treatable with oxygen or minor
airway support.
Ku conducted a small retrospective study on 17 neonatal ICU patients and
noted that IN midazolam and fentanyl were safe and effective in this
population.
Additional
studies note rapidly effective sedation to enhance ophthalmologic exam
in children and one study describes relief of anxiety surrounding minor
procedures such as venous blood sampling, IV catheter placement or
subcutaneous IV port access.[40-42, 202]
Sedation Literature Summary:
Summing up the literature, several general impressions can be stated. First, the three most commonly used intranasal sedation agents (midazolam, sufentanil, ketamine) all seem to have an effect in 5-10 minutes, peak in 12-20 minutes and become less effective after about 30-40 minutes though perhaps longer for higher doses of sufentanil. With the limited available evidence, it appears that a combination of midazolam plus sufentanil or midazolam plus ketamine achieves slightly more effective and deeper sedation than any alone. On the other hand, for simple induction of drowsiness for non-painful procedures such as MRI, a single agent such as midazolam at a low dose (0.2 mg/kg) is very effective. In terms of safety, it is very rare to see any desaturations with midazolam or ketamine. However, sufentanil in higher doses (> 1.5 mcg/kg) appears to have an increased incidence of nausea, vomiting, reduced respiratory rate and oxygen desaturation with occasional chest wall tightening described at dose ³ 2 mcg/kg - emphasizing the importance of careful monitoring with sufentanil therapy. Midazolam appears quite safe via the nasal route and it is an effective sedative and amnestic for minor procedures. It is also an effective alternative to oral formulations when patients refuse to swallow the oral dose. However it causes brief nasal mucosal burning following application. This burning may lead to crying immediately following application in children and parents must be forewarned to expect this initial response.
Schrier et al report pharmacokinetic data related to a new highly
concentrated from of Midazolam designed for IN delivery called Nazolam.[139]
It has 75% bioavailability, fairly rapid onset and good duration of
action and does not damage mucosa.
We can expect this to be on the market soon. It is a very well designed
product that will be prepackaged as single dose applicators making them
very convenient to administer and highly predictable in their effects.
If priced and marketed correctly these products should replace our
current techniques of using generic drugs. The question of course will
be affordability when compared to the less concentrated inexpensive
generic concentrations. Hopefully the manufacturers will find a middle
ground price structure where they make a fair profit and the price is
affordable so that widespread use occurs.
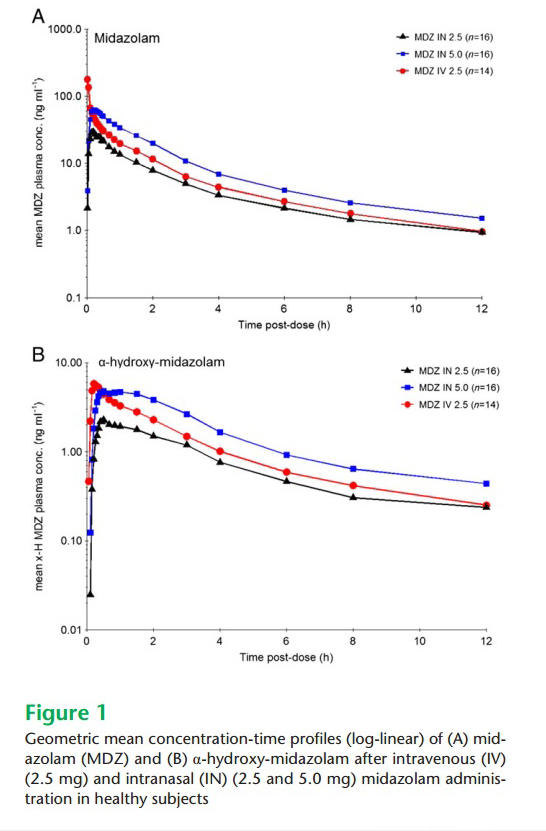
Schrier - Graph of midazolam concentration versus time profiles: This
graph demonstrates two important findings: First the high immediate peak
for IV midazolam but the lack of an immediate high peak concentration
for nasal midazolam – meaning the risk of respiratory depression is
minimal using the nasal drug. Second, nearly equivalent plasma levels of
nasal and IV drugs once the high risk high peak levels abate – meaning
similar sedative and anti-seizure effects regardless of which route of
delivery is chosen.
In addition to this discussion there is a separate discussion related to intranasal ketamine for sedation (including emergency patients) below.
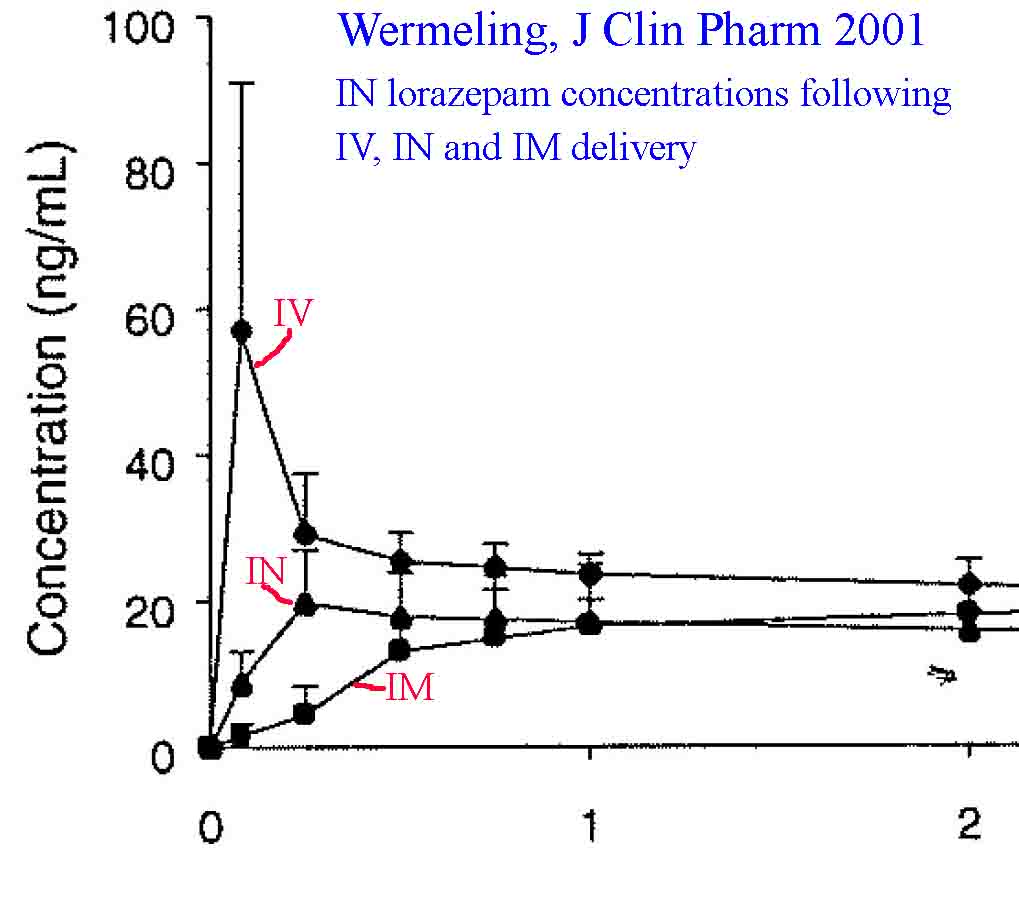
Agitated adults - sedation with intranasal haloperidol, midazolam or lorazepam
Acutely agitated patients present a dangerous situation to both themselves and to health care providers. For this reason, they are often physically restrained and provided pharmacologic sedation as soon as possible. Traditionally sedative is administered via an intramuscular shot because IV’s are notoriously difficult to establish and maintain, while oral therapy is usually refused by the patient. However, intramuscular administration of medications in these patients carries a substantial risk of needle stick injury to the health care provider - alternate routes of drug delivery would be useful. Too date, very little literature exists on this topic – perhaps due to the nearly impossible requirement of obtaining informed consent to conduct such a trial. Never the less there is some limited data to suggest that intranasal delivery of medications such as midazolam, lorazepam and haloperidol are effective. In 2004 Neff et al reported a small case series of adult ambulance patients (5 total) who were treated with intranasal midazolam (10 mg in 2 ml dose was their protocol) for acute agitation.[45] Despite failing to provide the entire dose as directed in 3/5 patients, they were still able to obtain resolution of the agitation 60% of the time. Manley et al showed adequate pre procedural sedation in > 90% of mentally disabled adults using a concentrated form of midazolam (40 mg/ml) and administering 10 mg to an adult - avoiding the need for general anesthesia in these situations (click here for article).[55]Lorazepam may also be effective in this situation. Wermeling et al reports lorazepam bioavailability at 78% when given intranasally,[46] and one of the web authors has used intranasal lorazepam in multiple acutely agitated patients (2 mg IN in adults) with about 70% effectiveness and fairly prolonged sedation (several hours).
Bregstein published a case report of a child with a violent behavioral
disorder who required chemical restraint but refused oral or buccal
medications. His mother asked for something other than an IM injection
due to his prior experiences with them and the fear they induced.
Furthermore the staff were concerned about needle stick risks given his
aggressive behavior. Therefore he was held down and administered 0.05
mg/kg of intranasal lorazepam. He was calm in 5 minutes and this lasted
about 3 hours. He required an additional dose which was increased to 0.1
mg/kg and this put him to sleep and kept him calm for hours.
Normandin report the utility of IN ketamine for sedating severely agitated ED patients - an attractive idea given the respiratory stable effects of Ketamine.[135] Cozzi et all suggest another use for IN dexmedetomidine: Anxiolysis in children with severe asthma exacerbations to allow better tolerance of their respiratory therapy without causing any respiratory depression.[140] Their report is only a case series but deserves further investigation. Finally, intranasal haloperidol may offer another option for intranasal sedation of acutely agitated adults. Miller et al report maximal serum levels of Haldol occurring in 15 minutes following intranasal delivery with rapid onset of sedation.[47] They conclude that intranasal haloperidol or other similar antipsychotic medications could play a role in treating psychiatric emergencies. Clearly all of this data is preliminary and would ideally undergo more rigorous research, but it does suggest an option (why not try first rather than risk a needle stick?) for EMS and ER providers to try before they move onto more invasive and dangerous treatment options.
Huebinger provide evidence from their EMS system (Chicago EMS) that demonstrate a midazolam protocol using either IN or IM midazolam (or occasionally IV) was a safe and effective method of calming agitated EMS patients.[229] Their initial dose was 5 mg IN/IM but they allowed a second dose if needed. The initial dose resulting in improvement in about 80% of cases with substantial improvement in 40%. When another dose was given, there was a similar degree of improvement yet again. There were very few adverse events – primarily nasal and oral discomfort (midazolam has a high pH so it burns on application).
Free internet article - Click here
Website manager Comments: Personally,
having reviewed the intranasal medication literature for over 20 years
and having used IN midazolam in my practice for a similar time period,
it is clear that clinicians tend to be overly conservative with nasal
drug dosing – fearing side effects like respiratory depression that they
have seen when the drug is given intravenously. With almost NO
exceptions, the use of generic IV midazolam (or fentanyl) via the nasal
route will NOT cause any substantial respiratory depression, it is
simply to dilute and is absorbed too slowly (a few minutes) to acutely
depress the respiratory drive. Therefore doses larger than an IV dose
are required to obtain a reliable clinical effect. The dose for sedation
in children is 0.4 to 0.5 mg/kg. Never the less, after over 30 years of
research on this dose, in children we still routinely see failed
sedation studies because of dosing in the 0.2 mg/kg range.
While I applaud these authors on the data obtained here, I can
vouch from extensive experience that their initial dose is less than
half of what it should be for an adult who is agitated. I would give 10
mg right up front (2 ml - more volume will just leak out their
nose). However, you need to realize that a 10 mg dose is less
than 0.15 mg/kg in a 70 kg adult so you will rarely see true sedation at
that dose. Titrate up as needed and anxiolysis and some calming is more
likely to occur. Sedation is highly unlikely.
Special Focus - Intranasal Ketamine for sedation
There is a growing interest in the effectiveness of
intranasal ketamine for pain control and for sedation. For insight into
the literature on pain control please
click here
to
move into the pain section of this web site where effectiveness of nasal
ketamine for pain is discussed. Below is an overview of the literature
that investigates nasal ketamine and its impact on sedation. The first
section summarizes the editors overall view of the evidence, the
remainder is a summary of each published article to date in
chronological order so you can make your own conclusions.
Summary
of evidence and insights regarding intranasal ketamine for
sedation:
About 20 studies are reviewed below and similar
patterns emerge from this data: Nasal ketamine is not 100% absorbed –
probably more in the 40-50% range with peak effects and blood levels at
about 20 minutes, so doses need to be adjusted upwards above the IV and
IM dose if ones goal is dissociative anesthesia. It is clear that doses
less than 5 mg/kg simply do not lead to reliable sedation – they may
cause anxiolysis, but they do not lead to depths of sedation adequate
for procedures beyond reducing separation anxiety.
Doses in the 5-6 mg/kg range do lead to some sedation, but rarely
dissociative anesthesia so once again they are not sufficiently reliable
for a painful procedural interventions in many children. Doses of 9-10
mg/kg do seem to reliably provide dissociative anesthesia levels of
sedation in children such that painful procedures are possible.
Unfortunately the majority of research to date does not use a dose this
high so we cannot be entirely clear how frequent this high dose will
fail. Interestingly the
authors of the original research on the topic in the 1980’s offer a
simple solution: Begin with a
moderate dose and volume – say 6 mg/kg intranasally, wait 10 minutes,
if you do not find dissociative
anesthesia and nystagmus to your liking, just administer an additional 3
mg/kg dose up to two additional times. Using this titrated effect the
authors established adequate procedural anesthesia in 98% of patient
within 15 minutes. This approach also offers a solution to the “volume”
issue of nasal drugs. You can administer more appropriate volumes (less
runoff and swallowing) if you titrate with several doses rather than
give a large nasal bolus all at once. Combination therapy with a
benzodiazepine or synthetic opiate may also be considered. A combination
of 6 mg/kg of ketamine plus 0.3 mg/kg of midazolam seems to achieve
fairly reliable sedation without respiratory depression in a number of
studies.
In summary, for mild sedation adequate to relieve
anxiety but not to conduct a painful procedure, use
a nasal ketamine dose of at least 5 mg/kg. If you actually intend
to do a painful or complex procedure you will need a dose in the 10
mg/kg range which can be achieved by either a single large dose, or by
initial administration of 6 mg/kg and 10 minutes later an additional 3-4
mg/kg. Dissociative anesthesia onset is usually within 5-15 minutes.
Combination therapy with
midazolam or sufentanil also seems quite effective and a lesser dose of
ketamine in the 5-6 mg/kg range is adequate when combined therapy is
provided.
Summary of
published articles - listed
chronologically:
Aldrete 1987:
Aldrete used a titrated dose of ketamine to induce preoperative sedation
in 42 children and compared that to a control group without sedation.[72] Using an initial dose of 3 mg/kg and progressing to as much as
9 mg/kg as needed the investigators were able to successfully perform
smooth mask induction in 41/42 children compared to only 22/42 in the
control arm. The onset of nystagmus and sedation was between 3 and 15
minutes (longer for those requiring titrated dosing).
Editorial
comment: It is unfortunate this study is only published as an abstract
so it is not more well known. This 25 years ago these authors recognized
that titration of drug was possible with nasal sedatives
– they gave a small dose of
ketamine (3 mg/kg) waited a few minutes and repeated with 1.5 to 3.0
mg/kg additional doses until the child was having nystagmus and
progressing to a more dissociative state. At that point they took the
child out of mothers’ arms and went to the operating room. Using this
titrated approach they were able to successfully deeply sedate 98% of
the cases. Too bad the next 25 years of research never repeated this
research design and instead locked themselves into a single often
inadequate dosing plan. Perhaps future researchers into intranasal
ketamine should consider this type of study design as most of us utilize
this approach with all other IV sedation techniques (IV benzos,
propofol, etc).
Aldrete 1988:
I am unable to access
this article so cannot review the information.
[73]
Lin 1990:
These authors compared placebo to intranasal ketamine (3 mg/kg) and
rectal ketamine (6 mg/kg) for preoperative anxiolysis.[74]
Based on their abstract (I cannot get the full article) they found that
the ketamine group tolerated mask induction better than the placebo
group.
Louon and
Reddy for 1992: These authors investigated a combination of
intranasal ketamine (5 mg/kg) plus midazolam (0.5 mg/kg) for use as a
mild sedative to calm children for pediatric computed tomography.[75]
The study was conducted in the early 1990’s when these tests routinely
lasted over an hour, so sedation was absolutely needed to obtain
adequate films. They dripped a quite high volume of drug into the
child’s nose over 5-10 minutes and then transferred them to CT when they
were asleep. This single non-titrated dose led to adequate mild sedation
(sleeping for a CT scan) in 83% of cases and there was no respiratory
depression.
Abrams 1993:
Abrams et al compared nasal ketamine 3 mg/kg to midazolam 0.4 mg/kg and
sufentanil 1.5 mcg/kg in children requiring sedation for minor dental
procedures.[76] In this early
research they diluted the drug with saline and they dripped it in with a
syringe (They mention a concern about OVER absorption and too strong of
an effect with atomization). They found that these doses of ketamine and
midazolam resulted in “acceptable” sedation (minor fussing, no struggle)
with rapid recovery while sufentanil at the dose they chose resulted in
over-sedation with oxygen desaturation and prolonged recovery.
Editorial
comment: Sufentanil at the doses used here will lead to sedation since
this opiate causes both pain control as well as sedation. Outpatient
studies from the emergency room suggest doses in the 0.5 mcg/kg range
are successful for pain control with little sedation, however this
editorialist has used nasal sufentanil extensively and found a number of
situations where mild sedation and even mild hypoxia (oxygen saturations
of 88%) will occur in the elderly at this lower dose. Children tend to
metabolize sufentanil more rapidly and effectively, but it is a very
powerful opiate and it is very lipophilic so it is not surprising that a
dose of 1.5 mcg/kg led to significant sedation.
Louon 1993:
This is a case report where the clinicians used a combination of
intranasal ketamine 6 mg/kg with midazolam 1 mg/kg to perform
cryotherapy on a premature baby suffering from retinopathy of
prematurity.[77] Due to the
concerns surrounding IV cannulation and general anesthesia they instead
chose rapid, brief sedation using the intranasal route. They found
combination nasal therapy very effective and safe
in this premature baby population and they did not see any
cardiopulmonary compromise.
Weksler
1993: This study compared intranasal ketamine 6 mg/kg to
intramuscular promethazine and meperidine (0.1 ml/kg of a mix containing
10 mg/ml of each drug).[78] 86
children were given ketamine and 62 the intramuscular drugs. Ketamine
sedation was excellent in 48, adequate in 19 and failed in 19 (22%).
Promethazine and meperidine induced sedation was excellent in 9,
adequate in 12 and failed in 41 (66%). The authors concluded that nasal
ketamine was an appropriate alternative to other routes of drug delivery
for preoperative sedation.
Malinovsky
1996: This study investigated
the pharmacokinetics of ketamine given as IV dose (3 mg.kg), nasal dose
(either 3 or 9 mg/kg) and rectal dose (9 mg/kg) in children who were
already under general anesthesia.[79]
The authors found that nasal ketamine peaks at 20 minutes while rectal
peaks at 42 minutes. Calculated bioavailability for the nasal drug was
50% while it was 25% for the rectal route.
Furthermore they found that 9 mg/kg of nasal ketamine resulted in
plasma levels comparable to the IV induction dose used to provide deep
anesthesia. The rectal drug pharmacokinetics were more like an oral drug
suggesting significant first pass metabolism of rectally delivered drug.
Editorial –
This early study goes a long ways towards helping us understand nasal
dosing of ketamine. Low doses in the 3 mg/kg range do not result in high
plasma levels so would not be expected to cause significant sedation,
though they are likely fine for pain control. Higher doses in the 9
mg/kg range achieve general anesthesia plasma levels. All future
clinical studies using nasal ketamine confirm these findings – doses
less than 5 mg/kg cause mild anxiolysis and good pain control but
little effective sedation, 5-6
mg/kg leads to fair sedation, while 9-10 mg/kg nasal doses lead to
deeper sedation. Future researchers could same themselves some effort
should they pay attention to these repeated dosing findings and consider
titration as was shown in Aldrete.
Diaz 1997:
This double blind RCT comparing IN ketamine 3 mg/kg in 2 ml
solution to saline for reducing separation anxiety and accepting the
mask in the operating theatre.[80]
While they did find a statistically significant improvement in overall
cooperation index compared to placebo, the clinical significance of this
score difference is unclear (5.4 vs 6.1 on a 4 to 12 scale – lower being
preferred) since it appears to be relatively small change in anxiety.
Editorial
comment - Once again – small doses of a drug that is not highly
bioavailable do not result in dramatic clinical effects such as
significant sedation.
Weber 2003:
This study randomized children scheduled for surgery into 3 groups and
investigated the efficacy of varying doses of nasal ketamine plus
midazolam or midazolam alone for preoperative sedation.[81]
The 3 groups (30 children each) received either ketamine 1 mg/kg plus
midazolam 0.2 mg/kg, ketamine 2 mg/kg plus midazolam 0.2 mg/kg, or
midazolam 0.2 mg/kg alone. They freely admit that their goal was simply
anxiolysis without deep sedation – they just wanted to dampen the stress
of separation from the parents. For this reason the doses they chose
were quite low and they never had deep sedation in any child. Although
they documented mild sedation/anxiolysis, there was little difference
between the groups - Basically
they found mildly better sedation in the higher combined dose of drug
over the lower or single drug regimen.
Yanagihara
2003: This is a small volunteer study looking at bioavailability
data when ketamine was delivered via multiple routes.[82]
Due to tiny sample size and unclear delivery techniques it is a bit
difficult to make firm conclusions. They found oral drug to be about 20%
bioavailable, sublingual and rectal 30% and nasal 45%. They recommend
the appropriate delivery route to match the clinical indication.
Weber 2004:
In this investigation the authors compared serum ketamine levels in
children who received 2 mg/kg of either IV ketamine or nasal ketamine.[83]
They found that IV levels peaked in the first three minutes whereas
nasal peaked in 18 minutes. They also noted that IV serum levels were
approximately 5 times higher than peak nasal drug levels (1860 vs 355 ng/ml)
and that at a dose of 2 mg/kg intranasally one would not expect
effective sedative levels of ketamine.
Roelofse
2004: These authors randomized 50 children undergoing multiple
dental extractions (6 or more teeth) to preoperative intranasal
sufentanil plus midazolam (1 mcg/kg plus 0.3 mg/kg) or intranasal
ketamine plus midazolam (5 mg/kg plus 0.3 mg/kg).[84]
They measured the preoperative acceptability of the spray, ease of mask
induction, anxiety score, sedation score, and post-operative pain score,
behavior score and any adverse reactions. In both groups they found the
drugs were easily delivered with an atomizer, had rapid onset with good
sedation and had easy mask induction and equivalent post-operative pain
control with no reported side effects. They conclude that either method
is acceptable and effective.
Editorial
comment: This study along with a few others suggest that one can achieve
adequate sedation with 5 mg/k of ketamine if at the same time a fairly
adequate dose of another sedative is also used.
Kazemi 2005:
Kazemi and colleagues randomized 130 preoperative patients to receive
either placebo, midazolam 0.2 mg/kg or Ketamine 5 mg/kg intranasally as
a sedative.[85] They found that
both active drugs resulted in equal amounts sedation and reduction in
reaction to IV cannulization. About 60% of the sedation was considered
“mild” while 20-30% was felt to be “good.” Both drugs were far superior
compared to placebo.
Editorial
comment – we already know that 0.2 mg/kg of midazolam is relatively
inadequate for sedation so these results are not surprising and
essentially confirm all prior literature on the topic. However, given
this study results we have one more bit of information suggesting that 5
mg/kg of intranasal ketamine alone is also barely adequate for sedation
– a conclusion confirmed by other studies. The study is quite well
designed in terms of randomization and placebo controlled so the results
are believable. The biggest errors noted that might have further
impacted drug efficacy are the fact that they diluted the drug to 2 ml
and dripped it in rather than aerosolized the drug.
Gharde 2006:
This randomized trial comparing intranasal ketamine to intranasal
midazolam or a combination of the two is one of the better trials
providing us insight into the effectiveness of intranasal ketamine for
this indication.[86] It is a good
trial because they actually used an appropriately high dose of ketamine
(10 mg/kg) to achieve success at both sedation and pain control. They
did make a pretty basic error in their midazolam dosing using a dose
well known to be fairly ineffective for sedation (0.2 mg/kg).
In this group of 60 children, the 40 who received nasal ketamine
all achieved excellent scores for sedation (3.75/4) and for tolerance of
separation (3.9/4) from parents and IV cannulation (3.9/4). Scores for
separation and cannulation in the midazolam cohort where significantly
lower. The authors conclude that intranasal ketamine was “excellent” for
separation and was probably more effective than midazolam because it
provides both sedation and pain control and therefore there was little
or no fussing when an IV cannula was started.
Berner 2007:
This is a report of a case noting anxiolysis and sedation in an adult
with psychiatric problems. The article provides an case relating to
successful use of intranasal ketamine for the treatment of refractory
intermittent explosive disorder, finding a dose of up to 60 mg effective
with use of over 200 mg in a day leading to some hallucinosis.[87]
Gautam 2007:
This study investigated IN midazolam 0.2 mg/kg vs. IN ketamine 5 mg/kg
for efficacy of preoperative sedation and reduction of separation
anxiety in 50 children. They found onset of good sedation in about 2/3
of patients in both groups at about 15 minutes time.[88]
Comment:
Again this is another study noting anxiolysis but not reliable sedation
at nasal ketamine doses in the 5 mg/kg range.
Pandey 2011:
This study investigated both the efficacy of intranasal ketamine for
sedation in uncooperative children undergoing dental procedures as well
as the relative acceptance of drop vs atomizer administered drug.[89] The authors studied 34 children in a cross-over model so each
child was their own control. 68 procedures were evaluated. They found
that intranasal ketamine at 6 mg/kg resulted in a goal of adequate
sedation in 91-97% and successful procedural efficacy in 85-94% of cases
(drops versus atomized). They found patient acceptance of nasal drug
delivery was far higher using the atomizer compared to drops (70%
excellent vs. 23% excellent, 6% poor versus 44% poor). These same
authors published additional data on 45 patients confirming the slightly
superior efficacy of IN ketamine over IN midazolam in another paper also
in the pediatric dental literature.[90]
Editorial –
Here is a paper suggesting that 6 mg/kg of intranasal ketamine is
adequate for moderate sedation in the vast majority of time in children.
Atomization is far superior to dropper application in terms of patient
acceptance.
Click here for the entire article
Tsze 2012:
This small emergency department study investigated the efficacy of
intranasal ketamine for sedation of children who required laceration
repair.[91] They randomized
children to doses of 3, 6 or 9 mg/kg in a blinded fashion. After
randomizing 12 patients they were required to suspend the study and
break the code due to 9 of 12 failures to sedate. They found that all
children who received 3 mg/kg or 6 mg/kg failed to achieve adequate
procedural sedation based on their predefined calculation using the
observations scale of behavioral distress (OSBD-R). They also measured
serum levels and found them considerably lower than those noted in the
Malinovsky paper from a few years prior. Three of 4 children receiving
the 9 mg/kg fentanyl dose were adequately sedated for suturing within
4-9 minutes. The authors conclude that in the emergency setting with
completely awake children, only the 9 mg/kg dose was effective for
sedation and that a larger trial using this higher dosing is needed to
determine actual efficacy and side effect profiles. One other
interesting bit of information reported by this article was the concept
that ketamine sedation is an on-off phenomenon and all that is needed is
an adequate serum level at which point the patient enters a phase of
dissociative anesthesia that is not further enhanced by more medication.
Therefore – if the adequate level can be achieved, the patient should
become dissociated. If this is true, then titration of dose via the
nose, as demonstrated 25 years earlier, would be an ideal way to
progress to adequate sedation in most children.
Hosseini
Jahromi 2012: These authors
randomized 120 children into 4 groups to determine the effectiveness of
intranasal medications for reducing preoperative separation anxiety.[92]
They used quite low doses of drug: 0.2 mg/kg of midazolam versus
0.5 mg/kg or 3 mg/kg of ketamine versus placebo. Not surprisingly they
found little efficacy though in this study they felt midazolam was
superior in causing sedation and reducing anxiety.
Editorial
comment: Having done a lot of research in my career and knowing how much
effort is expended for a few pages of print in a journal I find studies
like this a bit tragic. Based on over 20 years of prior studies the
results of this study are a forgone conclusion and the authors should
have known this when they wrote the study design. I only included it
here for completeness sake and to hope that other researchers might
notice these comments and results and not continue to make the same
mistakes when investigating nasal medications – if you fail to give a
therapeutic dose based on drug bioavailability, you will also fail to
find a positive result. This does not mean the concept is flawed, just
that you gave the wrong dose.
Miller 2015: Miller noted that IN
dexmedetomidine in doses of 2-3 mcg/kg were effective sedation for
pediatric transthoracic echo, of similar efficacy to oral choral
hydrate.
Intranasal flumazenil and intranasal naloxone as a reversal agents in sedated patients without an IV line
A concern that often comes up regarding administration of sedatives and opiates to patients who are given these powerful drugs via the intranasal route is how they can be reversed should too much sedation develop (since they presumably do not have an intravenous line). The first point that needs to be considered is whether significant respiratory depression requiring intervention beyond oxygen therapy will even occur from intranasal drug delivery. To date it has not been reported for midazolam and it does not even seem to occur with very high doses of the extremely powerful drug sufentanil. This is probably because the medications absorb via the nasal mucosa are spread out over 10-15 minutes and never achieve peak levels seen with intravenous boluses (see detailed discussion on therapeutic threshold and side effect threshold concept in the overview section and the pain medication section - click here). Never the less, antidotes to opiates - i.e. naloxone - work very well intranasally as well as via subcutaneous and intramuscular routes (see separate section on this topic - click here). In terms of intranasal flumazenil - the benzodiazepine antagonist - there is limited data but that which exists also suggests that it is effective when administered via the nasal route. Two animal studies found transmucosal flumazenil delivered via the sublingual route resulted in rapidly measurable serum drug levels that achieved the therapeutic threshold and approached 100% bioavailability.[48,49] One of these studies actually demonstrated reversal of benzodiazepine induced sedation about 4 minutes after drug delivery.[48] Two human studies exist in children using flumazenil intranasally Scheepers found maximal concentrations in the serum were achieved very quickly (2 minutes), again at therapeutic blood levels and concluded that this may offer an alternate delivery route for benzodiazepine antagonist reversal agents.[50] Heard presents a case where and child undergoing a dental procedure was over sedated using intranasal midazolam combined with intranasal sufentanil. [53] the authors responded to this problem by administering 0.4 on intranasal naloxone and 200 mcg of intranasal flumazenil. Three minutes following antidote administration the pati9ent was fully awake and did not become re-sedated during the next 2.5 hours of observation.
Personal insights from experienced clinicians
Doug Nelson, MD, Medical Director, Emergency Department, Primary Children's Medical Center, Salt Lake City, UT
We have been using the intranasal route for many years in our pediatric emergency department. Administering IN midazolam at a dose of 0.4 mg/kg results in effective sedation in >90% of children. More importantly we have never had a single adverse outcome in the literally thousands of children treated using this method.
Roni Lane, MD, Assistant Professor, Emergency Department, Primary Children's Medical Center, Salt Lake City, UT
I am one of 19 pediatric emergency medicine physicians practicing in a busy Level 1 Trauma center in a free standing children's hospital. We perform multiple sedations daily for a variety of procedures including closed fracture reduction, laceration repair, lumbar puncture, radiologic imaging and hernia reduction. Prior to the development of atomization devices, drip instillation of benzodiazepines frequently resulted in ineffective sedation with much of the medication lost to the oral cavity. For a number of years now, children undergoing minor procedures requiring sedation in our ED are given midazolam via a mucosal atomizer device resulting in successful sedation (anxiolysis) in 70-80% of patients. In addition, we use the mucosal atomizer device to deliver midazolam to patients who are seizing as well as fentanyl for some patients who are suffering from pain due to fractures. After thousands of sedations, we have noted no significant adverse events associated with midazolam administered in this fashion. With the exception of some nasal burning that occurs with administration, it is well tolerated. We are fortunate to have a method of providing effective light sedation in a fairly non-invasive fashion.
Mark Talon, MSN, CRNA, Department of Anesthesia, Shriners Hospital for Children, University of Texas Medical Branch - Galveston
The nasal atomizer has changed
our pediatric practice significantly. We have
been using IN therapy in many different fashions over the last several
years and have found dexmedetomidine to be a very valuable addition to
our premedications. As a sole medication for procedural sedation
dexmedetomidine is limited. Like clonidine the patient is easily
arousable yet sedate in a fashion similar to normal sleep. Thus as a
sole agent its effect is variable. Our practice for procedural sedation
with dexmedetomidine is to combine 2ug/kg of IN dexmedetomidine with
.5mg/kg of oral midazolam. This combination has proven to be far better
then either the Precedex or midazolam as a sole agent and usually
results in significant procedural sedation that allows us to remove burn
wound dressings, pins and often do casting and molding without further
intervention. We have used this method to sedate children for the MRI
and CT scanners without problems. This is also our standard
premedication for children less then 50kg going to surgery. The combined
effects are relatively consistent with the majority of children and
results in significant sedation in 30-40 minutes. Please realize that
the majority of our children are very anxious as they have been through
multiple surgeries and procedures for burn and reconstructive treatment,
so they have been exposed to many pharmacological mixes. In normal
children that have not been exposed to poly pharmacy the effects are
much more consistent. The duration of action is approximately 1.5 hours
at which point we see criteria that would meet discharge requirements.
We have also used combinations of intranasal opiates for sedation and
analgesia, but this is a much longer discussion.
Dan Tsze, MD; Assistant Professor, Hasbro Children's Hospital, Providence, RI
Our
pediatric emergency department is currently conducting a trial that
initially started by comparing three different doses of intranasal
ketamine for procedural sedation for laceration repairs: 3, 6, and 9
mg/kg. We decided to use
a mucosal atomizer to optimize nasal absorption and minimize the amount of solution
that might be swallowed instead.
We are utilizing the 100 mg/mL concentration, which was the
highest concentration we could obtain, to minimize the volume needed.
There is a 150 mg/mL concentration available from a
pharmaceutical company (but they did not want to participate in our
trial), as well as higher concentrations which were limited to
veterinary medicine.
The study
is double blinded, but we noticed that there was a large number of
clinical failures, meaning patients who did not achieve adequate
sedation within 30 minutes of drug administration.
Our safety committee reviewed the data while we remained blinded,
and made the recommendation to drop the 2 lower doses and consider
adding a higher dose(s) to the trial.
We revised the study and are now comparing 9 mg/kg and 12 mg/kg
doses. We are not
concurrently giving any midazolam or glycopyrrolate/atropine, and the
patients range from 1 to 7 years old.
We have limited the maximum dose to 300 mg (i.e. 3 mL), simply
for pragmatic reasons related to total volume and discomfort related to
intranasal administration.
As far as we can tell, while currently blinded, the time to onset of sedation has ranged anywhere from 6 minutes to just over 20 minutes. Patients who reached adequate sedation did not ever require "rescue" doses of additional ketamine to complete the laceration repairs, which were limited to simple lacerations less than 5 cm and did not require a consult service to perform the repair. Recovery times have been comparable to patients who have received IV ketamine. Unfortunately, since we are still blinded at this time, we cannot make any further comments regarding a specific dose and its effect.
Pat Crocker, DO, Chief of Emergency Medicine, Dell Children's Medical Center, Austin TX
We have had great success with IN fentanyl for immediate pain control in children and it is much quicker than waiting for an iv to be established. Giving the fentanyl IN immediately and applying some topical anesthetic cream makes subsequent iv insertion less traumatic for the child as well.
The combination of IN fentanyl and Versed prior to minor procedures and administration of local anesthetic has been quite useful as well. No child has fallen asleep at the suggested doses but generally is quite a bit more tractable for the procedure reducing our need for full sedations some. We have also combined the above with nitrous oxide for children 5 yo and older and get nice results.
Tom Macfarlane, MD, Emergency Physician, Salt lake City UT
Intranasal delivery of midazolam is an important niche therapy in my practice. I find it most useful in children who have a need for anxiolysis or light procedural sedation. I use it frequently for sedation in laceration repairs and in splinting of fractures that do not require reduction. Another common indication is light sedation for radiographic imaging. Onset is quite rapid and adverse events appear to be very rare. In addition patients are safe for discharge quite quickly thereby enhancing emergency department throughput. Overall I feel that this delivery route provides safe and effective light sedation in the emergency department.
Treatment protocol
General points:
-
Midazolam, ketamine, dexmedetomidine and sufentanil are the most commonly used
sedative medications for IN delivery.
-
Midazolam results in mild somnolence with resultant reduction in
anxiety and probably amnesia.
It will not make the patient unconscious.
-
Be aware that midazolam causes some nasal burning for
30-45 seconds when administered.
- In small children you should administer lidocaine 2% or 4% - 0.2 ml per nostril 5 minutes prior to the midazolam to stop the burning.
-
Be aware that midazolam causes some nasal burning for
30-45 seconds when administered.
-
Sufentanil will also cause deeper sedation and in doses over 1.5
mcg/kg has been noted to cause respiratory depression.
-
-
Midazolam results in mild somnolence with resultant reduction in
anxiety and probably amnesia.
It will not make the patient unconscious.
-
Combination therapy with midazolam plus
either sufentanil or ketamine may work better than any of the
medications alone
-
Newer data discussed above suggests that IN dexmedetomidine may be
the best option for sedation
-
Reasonable IN starting dose:
-
Midazolam 0.4 to 0.5 mg/kg
-
Use the lower dose
for minor, non-painful procedures such as radiographic
imaging
-
Use the higher dose
for better sedation prior to procedures such as laceration
repair
-
Use the lower dose
for minor, non-painful procedures such as radiographic
imaging
-
Ketamine 10 mg/kg
-
Sufentanil 1 to 1.5 mcg/kg
- Dexmedetomidine 2.5 to 3 mcg/kg
-
Combined dosing:
-
Midazolam plus
sufentanil: 0.2 to 0.3 mg/kg of midazolam plus 0.75 to 1
mcg/kg of sufentanil
-
Midazolam plus
ketamine: 0.2 to 0.3 mg/kg of midazolam plus 5 mg/kg of
ketamine
-
Midazolam plus
sufentanil: 0.2 to 0.3 mg/kg of midazolam plus 0.75 to 1
mcg/kg of sufentanil
-
Midazolam 0.4 to 0.5 mg/kg
-
Use only concentrated midazolam (5 mg/ml) and ketamine formulations
-
Be sure to monitor oxygen saturation in all patients
-
Ideal volume is 0.3 to 0.5 ml per nostril, maximum is 1 ml per
nostril, more will just run out nose.
- Nasal naloxone and flumazenil can be used as reversal agents
Dosing tables in Non-English language
Deutsch / German language
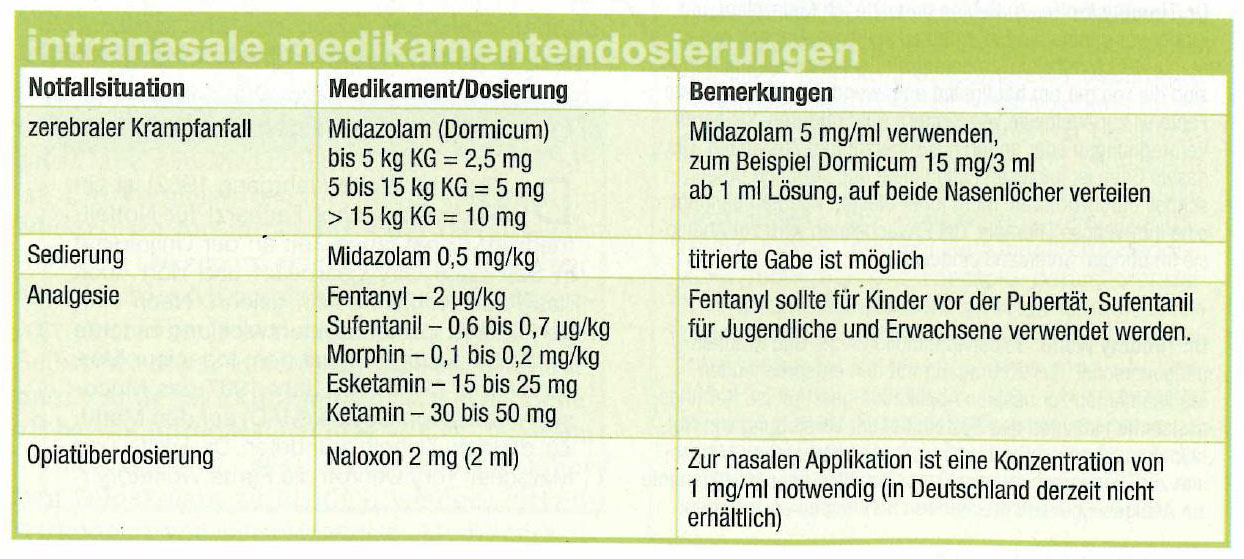{kind=link}
Deutsch 2 (Editors note: the doses are too low for fentanyl and morphine - double the dose these chart recommends for better effect that is still safe - see above literature)
Italia / Italian language
Teaching materials:
Peer Reviewed Articles -
Intranasal Midazolam for sedation
Al-Rakaf, Intra-nasal midazolam for conscious sedation of pediatric dental patients, Int J Ped Dentistry 2001 (click here) - PDF 0.32 MB
Manley, IN and IV midazolam for sedation in adults with learning disability, Br Dent Journal 2008
Morgans-Perri, MAD for IN midazolam pre-op, J Perianesthtic Nursing 2009 abstract
Intranasal ketamine for sedation
Kazemi, Intranasal ketamine versus intranasal midazolam for preoperative sedation in children, Pak J Med Sci 2005 (click here) - PDF 0.12 MB
Intranasal Dexmedetomidine for sedation and premedication before anesthesia
Detailed document describing IN Precedex for in hospital pediatric sedation for many situations
Bibliography (click here for abstracts)
1.
Abrams, R., et al., Safety and effectiveness of intranasal
administration of sedative medications (ketamine, midazolam, or
sufentanil) for urgent brief pediatric dental procedures. Anesth Prog,
1993. 40(3): p. 63-6.
2.
Roelofse, et al., Intranasal sufentanil/midazolam versus
ketamine/midazolam for analgesia/sedation in the pediatric population
prior to undergoing multiple dental extractions under general
anesthesia: a prospective, double-blind, randomized comparison. Anesth
Prog, 2004. 51(4): p. 114-21.
3.
Lee-Kim, S.J., et al., Nasal versus oral midazolam sedation for
pediatric dental patients. J Dent Child (Chic), 2004.
71(2): p. 126-30.
4.
Shashikiran, N.D., S.V. Reddy, and C.M. Yavagal, Conscious
sedation-An artist's science! An Indian experience with midazolam. J
Indian Soc Pedod Prev Dent, 2006.
24(1): p. 7-14.
5.
Primosch, R.E. and F. Bender, Factors associated with
administration route when using midazolam for pediatric conscious
sedation. ASDC J Dent Child, 2001.
68(4): p. 233-8, 228.
6.
Fuks, A.B., et al., Assessment of two doses of intranasal
midazolam for sedation of young pediatric dental patients. Pediatr Dent,
1994. 16(4): p. 301-5.
7.
Fukuta, O., et al., The sedative effect of intranasal midazolam
administration in the dental treatment of patients with mental
disabilities. Part 1. The effect of a 0.2 mg/kg dose. J Clin Pediatr
Dent, 1993. 17(4): p. 231-7.
8.
Fukuta, O., et al., The sedative effects of intranasal midazolam
administration in the dental treatment of patients with mental
disabilities. Part 2: optimal concentration of intranasal midazolam. J
Clin Pediatr Dent, 1994. 18(4):
p. 259-65.
9.
Gilchrist, F., A.M. Cairns, and J.A. Leitch, The use of
intranasal midazolam in the treatment of paediatric dental patients.
Anaesthesia, 2007. 62(12): p.
1262-5.
10.
Hartgraves, P.M. and R.E. Primosch, An evaluation of oral and
nasal midazolam for pediatric dental sedation. ASDC J Dent Child, 1994.
61(3): p. 175-81.
11.
Kaufman, E., et al., Comparison between intranasal and
intravenous midazolam sedation (with or without patient control) in a
dental phobia clinic. J Oral Maxillofac Surg, 1994.
52(8): p. 840-3; discussion
844.
12.
Shapira, J., et al., The effectiveness of midazolam and
hydroxyzine as sedative agents for young pediatric dental patients. ASDC
J Dent Child, 1996. 63(6): p.
421-5.
13.
Dallman, J.A., M.A. Ignelzi, Jr., and D.M. Briskie, Comparing the
safety, efficacy and recovery of intranasal midazolam vs. oral chloral
hydrate and promethazine. Pediatr Dent, 2001.
23(5): p. 424-30.
14.
Acworth, J.P., D. Purdie, and R.C. Clark, Intravenous ketamine
plus midazolam is superior to intranasal midazolam for emergency
paediatric procedural sedation. Emerg Med J, 2001.
18(1): p. 39-45.
15.
Bates, B.A., S.A. Schutzman, and G.R. Fleisher, A comparison of
intranasal sufentanil and midazolam to intramuscular meperidine,
promethazine, and chlorpromazine for conscious sedation in children. Ann
Emerg Med, 1994. 24(4): p. 646-51.
16.
Yealy, D.M., et al., Intranasal midazolam as a sedative for
children during laceration repair. Am J Emerg Med, 1992.
10(6): p. 584-7.
17.
Theroux, M.C., et al., Efficacy of intranasal midazolam in
facilitating suturing of lacerations in preschool children in the
emergency department. Pediatrics, 1993.
91(3): p. 624-7.
18.
Everitt, I.J. and P. Barnett, Comparison of two benzodiazepines
used for sedation of children undergoing suturing of a laceration in an
emergency department. Pediatr Emerg Care, 2002.
18(2): p. 72-4.
19.
Malinovsky, J.M., et al., Premedication with midazolam in
children. Effect of intranasal, rectal and oral routes on plasma
midazolam concentrations. Anaesthesia, 1995.
50(4): p. 351-4.
20.
Bayrak, F., et al., A comparison of oral midazolam, oral
tramadol, and intranasal sufentanil premedication in pediatric patients.
J Opioid Manag, 2007. 3(2):
p. 74-8.
21.
Karl, H.W., et al., Comparison of the safety and efficacy of
intranasal midazolam or sufentanil for preinduction of anesthesia in
pediatric patients. Anesthesiology, 1992.
76(2): p. 209-15.
22.
Zedie, N., et al., Comparison of intranasal midazolam and
sufentanil premedication in pediatric outpatients. Clin Pharmacol Ther,
1996. 59(3): p. 341-8.
23.
Weber, et al., Premedication with nasal s-ketamine and midazolam
provides good conditions for induction of anesthesia in preschool
children. Can J Anaesth, 2003. 50(5):
p. 470-5.
24.
Weber, et al., S-ketamine and s-norketamine plasma concentrations
after nasal and i.v. administration in anesthetized children. Paediatr
Anaesth, 2004. 14(12): p.
983-8.
25.
Weksler, N., et al., Nasal ketamine for paediatric premedication.
Can J Anaesth, 1993. 40(2):
p. 119-21.
26.
Malinovsky, J.M., et al., Plasma concentrations of midazolam
after i.v., nasal or rectal administration in children. Br J Anaesth,
1993. 70(6): p. 617-20.
27.
Otsuka, Y., et al., [Intranasal midazolam for sedation before
anesthesia in pediatric patients]. Masui, 1994.
43(1): p. 106-10.
28.
Rose, E., D. Simon, and J.P. Haberer, [Premedication with
intranasal midazolam in pediatric anesthesia]. Ann Fr Anesth Reanim,
1990. 9(4): p. 326-30.
29.
Saint-Maurice, C., et al., The use of midazolam in diagnostic and
short surgical procedures in children. Acta Anaesthesiol Scand Suppl,
1990. 92(1): p. 39-41.
30.
Vivarelli, R., et al., [Premedication with intranasal midazolam
in children of various ages]. Minerva Anestesiol, 1998.
64(11): p. 499-504.
31.
Karl, H.W., et al., Transmucosal administration of midazolam for
premedication of pediatric patients. Comparison of the nasal and
sublingual routes. Anesthesiology, 1993.
78(5): p. 885-91.
32.
Khazin, V., S. Ezra, and A. Cohen, Comparison of rectal to
intranasal administration of midazolam for premedication of children.
Mil Med, 1995. 160(11): p. 579-81.
33.
Kogan, A., et al., Premedication with midazolam in young
children: a comparison of four routes of administration. Paediatr
Anaesth, 2002. 12(8): p. 685-9.
34.
Hollenhorst, J., et al., Using intranasal midazolam spray to
prevent claustrophobia induced by MR imaging. AJR Am J Roentgenol, 2001.
176(4): p. 865-8.
35.
Tschirch, F.T., et al., Low-dose intranasal versus oral midazolam
for routine body MRI of claustrophobic patients. Eur Radiol, 2007.
17(6): p. 1403-10.
36.
Louon, A. and V.G. Reddy, Nasal midazolam and ketamine for
paediatric sedation during computerised tomography. Acta Anaesthesiol
Scand, 1994. 38(3): p. 259-61.
37.
Harcke, H.T., L.E. Grissom, and M.A. Meister, Sedation in
pediatric imaging using intranasal midazolam. Pediatr Radiol, 1995.
25(5): p. 341-3.
38.
Fishbein, M., et al., Evaluation of intranasal midazolam in
children undergoing esophagogastroduodenoscopy. J Pediatr Gastroenterol
Nutr, 1997. 25(3): p. 261-6.
39.
Uygur-Bayramicli, O., et al., Sedation with intranasal midazolam
in adults undergoing upper gastrointestinal endoscopy. J Clin
Gastroenterol, 2002. 35(2): p. 133-7.
40.
Gobeaux, D., et al., [Intranasal midazolam in pediatric
ophthalmology]. Cah Anesthesiol, 1991.
39(1): p. 34-6.
41.
Louon, A., et al., Sedation with nasal ketamine and midazolam for
cryotherapy in retinopathy of prematurity. Br J Ophthalmol, 1993.
77(8): p. 529-30.
42.
Ljungman, G., et al., Midazolam nasal spray reduces procedural
anxiety in children. Pediatrics, 2000.
105(1 Pt 1): p. 73-8.
43. Yuen, V.M., et al., A comparison of intranasal dexmedetomidine and oral midazolam for premedication in pediatric anesthesia: a double-blinded randomized controlled trial. Anesth Analg, 2008. 106(6): p. 1715-21.
44. Stella, M.J. and A.G. Bailey, Intranasal clonidine as a premedicant: three cases with unique indications. Paediatr Anaesth, 2008. 18(1): p. 71-3.45. Neff, C., S.M. Joyce, and A. Allred, Efficacy and safety of intranasal midazolam administration by EMS personnel for seizures and sedation. NAEMSP Winter abstracts, 2006.
46. Wermeling, D.P., et al., Bioavailability and pharmacokinetics of lorazepam after intranasal, intravenous, and intramuscular administration. J Clin Pharmacol, 2001. 41(11): p. 1225-31.
47. Miller, J.L., et al., Comparison of intranasal administration of haloperidol with intravenous and intramuscular administration: A pilot pharmacokinetic study. Pharmacotherapy, 2008. 28(7): p. 875-882.
48. Heniff, M.S., et al., Comparison of routes of flumazenil administration to reverse midazolam-induced respiratory depression in a canine model. Acad Emerg Med, 1997. 4(12): p. 1115-8.
49. Oliver, F.M., et al., Comparative pharmacokinetics of submucosal vs. intravenous flumazenil (Romazicon) in an animal model. Pediatr Dent, 2000. 22(6): p. 489-93.
50. Scheepers, L.D., et al., Plasma concentration of flumazenil following intranasal administration in children. Can J Anaesth, 2000. 47(2): p. 120-4.
51. Talon, M.D., et al., Intranasal Dexmedetomidine Premedication is Comparable With Midazolam in Burn Children Undergoing Reconstructive Surgery. J Burn Care Res, 2009. 30(4): p. 599-605.
56. Sakurai, Y., et al., Buccal administration of dexmedetomidine as a preanesthetic in children. J Anesth, 2010. 24(1): p. 49-53.
57. Wood, M., The safety and efficacy of intranasal midazolam sedation combined with inhalation sedation with nitrous oxide and oxygen in paediatric dental patients as an alternative to general anaesthesia. SAAD Dig, 2010. 26: p. 12-22.
58. Ransford NJ, Manley MC, Lewis DA, Thompson SA, Wray LJ, Boyle CA, et al. Intranasal/intravenous sedation for the dental care of adults with severe disabilities: a multicentre prospective audit. Br Dent J 2010;208(12):565-9.
59. Yuen VM, Hui TW, Irwin MG, Yao TJ, Wong GL, Yuen MK. Optimal timing for the administration of intranasal dexmedetomidine for premedication in children. Anaesthesia 2010.
60. Mukherjee, S., et al., Clonidine Premedication for Paediatric Patients: A comparison of the oral & nasal route. J Anaesth Clin Pharmacol, 2010. 26(3): p. 319-322.
61. Chiaretti, A., G. Barone, et al. (2010). "Intranasal lidocaine and midazolam for procedural sedation in children." Arch Dis Child.
62. Cheung, C.W., et al., Analgesic and sedative effects of intranasal dexmedetomidine in third molar surgery under local anaesthesia. Br J Anaesth, 2011. 107(3): p. 430-7.
63. Klein, E.J., et al., A Randomized Clinical Trial Comparing Oral, Aerosolized Intranasal, and Aerosolized Buccal Midazolam. Ann Emerg Med, 2011.
67. Iirola, T., et al., Bioavailability of dexmedetomidine after intranasal administration. Eur J Clin Pharmacol, 2011. 67(8): p. 825-31.
68. Kawanda, L., et al., Sedation with intranasal midazolam of Angolan children undergoing invasive procedures. Acta Paediatr, 2012. 101(7): p. e296-8.
69. Akin, A., A. Bayram, et al. (2012). "Dexmedetomidine vs
midazolam for premedication of pediatric patients undergoing
anesthesia." Paediatr Anaesth
22(9): 871-876.
70. Antonio, C., J. Zurek, et al.
(2011). "Reducing the pain of intranasal drug administration."
Pediatr Dent 33(5):
415-419.
71. Ozen, B., S. F. Malamed, et
al. (2012). "Outcomes of moderate sedation in paediatric dental
patients." Aust Dent J 57(2):
144-150.
72. Aldrete, J.A., et al.,
Intranasal Ketamine as induction adjunct in children: Preliminary
report. Anesthesiology, 1987.
67(3): p. A514.
73.
Aldrete, J.A., L.J. Russell, and F.A. Davis,
Intranasal administration of
ketamine: possible applications. Acta Anaesthesiol Belg, 1988.
39(3): p. 95-6.
74.
Lin, S.M., et al., Rectal ketamine
versus intranasal ketamine as premedicant in children. Ma Tsui Hsueh
Tsa Chi, 1990. 28(2): p.
177-83.
75.
Louon, A. and V.G. Reddy, Nasal midazolam and ketamine for paediatric sedation during computerised
tomography. Acta Anaesthesiol Scand, 1994.
38(3): p. 259-61.
76.
Abrams, R., et al., Safety
and effectiveness of intranasal administration of sedative medications
(ketamine, midazolam, or sufentanil) for urgent brief pediatric dental
procedures. Anesth Prog, 1993.
40(3): p. 63-6
77. Louon, A., et al.,
Sedation with nasal ketamine and midazolam for cryotherapy in
retinopathy of prematurity. Br J Ophthalmol, 1993.
77(8): p. 529-30.
78.
Weksler, N., et al., Nasal
ketamine for paediatric premedication. Can J Anaesth, 1993.
40(2): p. 119-21.
79.
Malinovsky, J.M., et al., Ketamine and norketamine plasma concentrations after i.v., nasal and
rectal administration in children. Br J Anaesth, 1996.
77(2): p. 203-7.
80.
Diaz, J.H., Intranasal ketamine
preinduction of paediatric outpatients. Paediatr Anaesth, 1997.
7(4): p. 273-8.
81. Weber, et al.,
Premedication with nasal
s-ketamine and midazolam provides good conditions for induction of
anesthesia in preschool children. Can J Anaesth, 2003.
50(5): p. 470-5.
82. Yanagihara, et
al., Plasma concentration profiles
of ketamine and norketamine after administration of various ketamine
preparations to healthy Japanese volunteers. Biopharm Drug Dispos,
2003. 24(1): p. 37-43.
83. Weber, et al.,
S-ketamine and s-norketamine
plasma concentrations after nasal and i.v. administration in
anesthetized children. Paediatr Anaesth, 2004.
14(12): p. 983-8.
84. Roelofse, J.A.,
et al., Intranasal
sufentanil/midazolam versus ketamine/midazolam for analgesia/sedation in
the pediatric population prior to undergoing multiple dental extractions
under general anesthesia: a prospective, double-blind, randomized
comparison. Anesth Prog, 2004.
51(4): p. 114-21.
85. Kazemi, A.P.,
H. Kamaliopour, and M. Seddighi,
Comparison of intranasal midazolam versus ketamine as premedication in
2-5 years old paeditric surgery patients. Pak J Med Sci, 2005.
21(4): p. 460-464.
86. Gharde, P., S.
Chauhan, and U. Kiran, Evaluation of efficacy of intranasal midazolam, ketamine and their
mixture as premedication and its relation with bispectral index in
children with tetralogy of fallot undergoing intracardiac repair.
Ann Card Anaesth, 2006. 9(1):
p. 25-30.
87. Berner, J.E.,
Intranasal ketamine for
intermittent explosive disorder: a case report. J Clin Psychiatry,
2007. 68(8): p. 1305.
88. Gautam, S.N.,
et al., Intranasal midazolam Vs
ketamine as premedication in paediatric surgical procedure for child
separation and induction. Nepal Med Coll J, 2007.
9(3): p. 179-81.
89. Pandey, R.K.,
et al., A comparative evaluation
of drops versus atomized administration of intranasal ketamine for the
procedural sedation of young uncooperative pediatric dental patients: a
prospective crossover trial. J Clin Pediatr Dent, 2011.
36(1): p. 79-84.
90. Bahetwar, S.K.,
et al., A comparative evaluation
of intranasal midazolam, ketamine and their combination for sedation of
young uncooperative pediatric dental patients: a triple blind randomized
crossover trial. J Clin Pediatr Dent, 2011.
35(4): p. 415-20.
91. Tsze, D.S., et
al., Intranasal Ketamine for
Procedural Sedation in Pediatric Laceration Repair: A Preliminary
Report. Pediatr Emerg Care, 2012.
28(8): p. 767-770.
92.
Hosseini Jahromi, S.A., et al.,
Comparison of the effects of
intranasal midazolam versus different doses of intranasal ketamine on
reducing preoperative pediatric anxiety: a prospective randomized
clinical trial. J Anesth, 2012.
94.
Nooh, N., S. A.
Sheta, et al. (2013). "Intranasal atomized dexmedetomidine for sedation
during third molar extraction." Int J Oral Maxillofac Surg
42(7): 857-862.
95. Papolos, D. F., M. H. Teicher, et al. (2013). "Clinical
experience using intranasal ketamine in the treatment of pediatric
bipolar disorder/fear of harm phenotype." J Affect Disord
147(1-3): 431-436.
96. Acker, A. and M.A. Jamieson,
Use of intranasal midazolam for
manual separation of labial adhesions in the office. J Pediatr
Adolesc Gynecol, 2013. 26(3): p. 196-8.
99. Jayaraman, L., A. Sinha,
et al. (2013). "A comparative study to evaluate the effect of intranasal
dexmedetomidine versus oral alprazolam as a premedication agent in
morbidly obese patients undergoing bariatric surgery." J Anaesthesiol
Clin Pharmacol 29(2):
179-182.
100.
Filho, E. M., W. B. de Carvalho, et al. (2013). "Aerosolized intranasal
midazolam for safe and effective sedation for quality computed
tomography imaging in infants and children." J Pediatrics
163: 1217-1219.
101. Mitra, S., S. Kazal,
et al. (2013). "Intranasal clonidine vs midazolam as premedication in
children: A randomized controlled trial." Indian Pediatr (In
press).
107. Nielsen, B. N., S. M. Friis, et al. (2014). "Intranasal
sufentanil/ketamine analgesia in children." Paediatr Anaesth
24(2): 170-180.
113. Patel, V.J., et al., Vasovagal syncope and severe bradycardia following intranasal dexmedetomidine for pediatric procedural sedation. Paediatr Anaesth, 2014. 24(4): p. 446-8.
114. Savla, J.R., et al., Effect of intranasal dexmedetomidine or oral midazolam premedication on sevoflurane EC50 for successful laryngeal mask airway placement in children: a randomized, double-blind, placebo-controlled trial. Paediatr Anaesth, 2014. 24(4): p. 433-9.
115. Xu, Y., X. Song, and G. Zhang, [ED50 of dexmedetomidine nasal drip in induction of hypnosis in children during computed tomography]. Zhonghua Yi Xue Za Zhi, 2014. 94(24): p. 1886-8.
116. Yao, Y., et al., Intranasal dexmedetomidine premedication reduces the minimum alveolar concentration of sevoflurane for tracheal intubation in children: a randomized trial. J Clin Anesth, 2014. 26(4): p. 309-14.
117. Surendar, M.N., et al., A comparative evaluation of intranasal dexmedetomidine, midazolam and ketamine for their sedative and analgesic properties: a triple blind randomized study. J Clin Pediatr Dent, 2014. 38(3): p. 255-61.
118. Cheung CW, Qiu Q, Liu J, Chu KM, Irwin MG. Intranasal dexmedetomidine in combination with patient-controlled sedation during upper gastrointestinal endoscopy: a randomised trial. Acta Anaesthesiol Scand 2015;59:215-23.
119. Mekitarian Filho E, Robinson F, de Carvalho WB, Gilio AE, Mason KP. Intranasal Dexmedetomidine for Sedation for Pediatric Computed Tomography Imaging. J Pediatr 2015.
120. Mukherjee A, Das A, Basunia SR, Chattopadhyay S, Kundu R, Bhattacharyya R. Emergence agitation prevention in paediatric ambulatory surgery: A comparison between intranasal Dexmedetomidine and Clonidine. Journal of research in pharmacy practice 2015;4:24-30.
121. Musani, I. E. and N. V. Chandan (2015). "A comparison of the sedative
effect of oral versus nasal midazolam combined with nitrous oxide in
uncooperative children." Eur Arch Paediatr Dent.
122. Fallahinejad Ghajari, M., G. Ansari, et al. (2015). "Comparison of
Oral and Intranasal Midazolam/Ketamine Sedation in 3-6-year-old
Uncooperative Dental Patients." J Dent Res Dent Clin Dent Prospects
9(2): 61-65.
123. Eskandarian, T., S. Arabzade Moghadam, et al. (2015). "The effect of
nasal midazolam premedication on parents-child separation and recovery
time in dental procedures under general anaesthesia." Eur J Paediatr
Dent 16(2): 135-138.
124. Shrestha, G. S., P. Joshi, et al. (2015). "Intranasal midazolam for
rapid sedation of an agitated patient." Indian J Crit Care Med
19(6): 356-358.
125. Montero, J. V., E. M. Nieto, et al. (2015). "Intranasal midazolam for
the emergency management of hypercyanotic spells in tetralogy of fallot."
Pediatr Emerg Care 31(4):
269-271.
127. Li, B. L., J. Ni, et al. (2015). "Intranasal dexmedetomidine for
sedation in children undergoing transthoracic echocardiography study-a
prospective observational study." Paediatr Anaesth
25(9): 891-896.
129. Yao, Y., B. Qian, et al. (2015). "Intranasal dexmedetomidine
premedication reduces minimum alveolar concentration of sevoflurane for
laryngeal mask airway insertion and emergence delirium in children: a
prospective, randomized, double-blind, placebo-controlled trial."
Paediatr Anaesth 25(5):
492-498.
133. Narendra, P. L., R. W.
Naphade, et al. (2015). "A comparison of intranasal ketamine and
intranasal midazolam for pediatric premedication." Anesth Essays Res
9(2): 213-218.
134. Miller, J., B. Xue, et al.
(2015). "Comparison of dexmedetomidine and chloral hydrate sedation for
transthoracic echocardiography in infants and toddlers: a randomized
clinical trial." Paediatr Anaesth.
135. Normandin, P. A., S. J. Khorey, et
al. (2015). "Use of Intranasal Ketamine for the Severely Agitated or
Violent ED Patient." J Emerg Nurs.
136. Greaves, A. (2016). "The use of Midazolam as an Intranasal Sedative
in Dentistry." SAAD Dig 32: 46-49.
137. Neville, D. N., K. R. Hayes, et al. (2016). "Double-blind
Randomized Controlled Trial of Intranasal Dexmedetomidine Versus
Intranasal Midazolam as Anxiolysis Prior to Pediatric Laceration Repair
in the Emergency Department." Acad Emerg Med
23(8): 910-917.
139.
Schrier, L., R. Zuiker, et al. (2017). "Pharmacokinetics and
pharmacodynamics of a new highly concentrated intranasal midazolam
formulation for conscious sedation." Br J Clin Pharmacol
83(4): 721-731.
140.
Shanmugaavel, A. K., S. Asokan, et al. (2016). "Comparison of Drug
Acceptance and Anxiety Between Intranasal and Sublingual Midazolam
Sedation." Pediatr Dent 38(2): 106-111.
141.
Smith, D., H. Cheek, et al. (2017). "Lidocaine Pretreatment Reduces the
Discomfort of Intranasal Midazolam Administration: A Randomized,
Double-blind, Placebo-controlled Trial." Acad Emerg Med
24(2): 161-167.
142.
Baier, N. M., S. S. Mendez, et al. (2016). "Intranasal dexmedetomidine:
an effective sedative agent for electroencephalogram and auditory brain
response testing." Paediatr Anaesth
26(3): 280-285.
143.
Bhat, R., M. C. Santhosh, et al. (2016). "Comparison of intranasal
dexmedetomidine and dexmedetomidine-ketamine for premedication in
pediatrics patients: A randomized double-blind study." Anesth Essays
Res 10(2): 349-355.
144.
Cozzi, G., S. Lega, et al. (2016). "Intranasal Dexmedetomidine Sedation
as Adjuvant Therapy in Acute Asthma Exacerbation With Marked Anxiety and
Agitation." Ann Emerg Med.
145.
Gan, X., H. Lin, et al. (2016). "Rescue Sedation With Intranasal
Dexmedetomidine for Pediatric Ophthalmic Examination After Chloral
Hydrate Failure: A Randomized, Controlled Trial." Clin Ther
38(6): 1522-1529.
146.
Ghai, B., K. Jain, et al. (2016). "Comparison of oral midazolam with
intranasal dexmedetomidine premedication for children undergoing CT
imaging: a randomized, double-blind, and controlled study." Paediatr
Anaesth.
147.
Lu, C., L. M. Zhang, et al. (2016). "Intranasal Dexmedetomidine as a
Sedative Premedication for Patients Undergoing Suspension Laryngoscopy:
A Randomized Double-Blind Study." PLoS One
11(5): e0154192.
148.
Wu, X., L. H. Hang, et al. (2016). "Intranasally Administered Adjunctive
Dexmedetomidine Reduces Perioperative Anesthetic Requirements in General
Anesthesia." Yonsei Med J
57(4): 998-1005.
149.
Malhotra, P. U., S. Thakur, et al. (2016). "Comparative evaluation of
dexmedetomidine and midazolam-ketamine combination as sedative agents in
pediatric dentistry: A double-blinded randomized controlled trial."
Contemp Clin Dent 7(2):
186-192.
150.
Miller, J. W., A. A. Divanovic, et al. (2016). "Dosing and efficacy of
intranasal dexmedetomidine sedation for pediatric transthoracic
echocardiography: a retrospective study." Can J Anaesth
63(7): 834-841.
151.
Sidhu, G. K., S. Jindal, et al. (2016). "Comparison of Intranasal
Dexmedetomidine with Intranasal Clonidine as a Premedication in
Surgery." Indian J Pediatr.
152.
Zhang, W., Y. Fan, et al. (2016). "Median Effective Dose of Intranasal
Dexmedetomidine for Rescue Sedation in Pediatric Patients Undergoing
Magnetic Resonance Imaging." Anesthesiology.
153.
Zhang, W., Z. Wang, et al. (2016). "Comparison of rescue techniques for
failed chloral hydrate sedation for magnetic resonance imaging
scans--additional chloral hydrate vs intranasal dexmedetomidine."
Paediatr Anaesth 26(3): 273-279.
154.
AlSarheed, M. A. (2016). "Intranasal sedatives in pediatric dentistry."
Saudi Med J 37(9):
948-956.
155. Behrle, N., E. Birisci, et al. (2017).
"Intranasal Dexmedetomidine as a Sedative for Pediatric Procedural
Sedation." J Pediatr Pharmacol Ther
22(1):
4-8.
156. Cao, Q., Y. Lin, et al. (2017). "Comparison of sedation by intranasal
dexmedetomidine and oral chloral hydrate for pediatric ophthalmic
examination." Paediatr Anaesth
27(6): 629-636.
157. Cozzi, G., S. Norbedo, et al. (2017). "Intranasal Dexmedetomidine for
Procedural Sedation in Children, a Suitable Alternative to Chloral
Hydrate." Paediatr Drugs
19(2): 107-111.
158. El-Hamid, A. M. A. and H. M. Yassin (2017). "Effect of intranasal
dexmedetomidine on emergence agitation after sevoflurane anesthesia in
children undergoing tonsillectomy and/or adenoidectomy." Saudi J
Anaesth 11(2): 137-143.
159. Kumar, L., A. Kumar, et al. (2017). "Efficacy of intranasal
dexmedetomidine versus oral midazolam for paediatric premedication."
Indian J Anaesth 61(2):
125-130.
160. Yuen, V. M., B. L. Li, et
al. (2017). "A randomised controlled trial of oral chloral hydrate vs.
intranasal dexmedetomidine before computerised tomography in children."
Anaesthesia 72(10): 1191-1195.
161. Ghai, B., K. Jain, et al. (2017). "Comparison of
oral midazolam with intranasal dexmedetomidine premedication for
children undergoing CT imaging: a randomized, double-blind, and
controlled study." Paediatr Anaesth
27(1): 37-44.
162. Gupta, A., N. P. Dalvi, et al. (2017). "Comparison between intranasal
dexmedetomidine and intranasal midazolam as premedication for brain
magnetic resonance imaging in pediatric patients: A prospective
randomized double blind trial." J Anaesthesiol Clin Pharmacol
33(2): 236-240.
163. Sulton, C., P. Kamat, et
al. (2017). "The Use of Intranasal Dexmedetomidine and Midazolam for
Sedated Magnetic Resonance Imaging in Children: A Report From the
Pediatric Sedation Research Consortium."
Pediatr Emerg Care.
164. Cozzi, G., S. Lega, et al. (2017). "Intranasal Dexmedetomidine
Sedation as Adjuvant Therapy in Acute Asthma Exacerbation With Marked
Anxiety and Agitation." Ann Emerg Med
69(1): 125-127.
165. Liu, Y., Q. Yu, et al. (2017). "Median effective
dose of intranasal dexmedetomidine sedation for transthoracic
echocardiography examination in postcardiac surgery and normal children:
An up-and-down sequential allocation trial." Eur J Anaesthesiol.
166. Yu, Q., Y. Liu, et al. (2017). "Median effective dose of intranasal
dexmedetomidine sedation for transthoracic echocardiography in pediatric
patients with noncyanotic congenital heart disease: An up-and-down
sequential allocation trial." Paediatr Anaesth
27(11): 1108-1114.
167. Mellion, S. A., D. Bourne, et al. (2017). "Evaluating Clinical
Effectiveness and Pharmacokinetic Profile of Atomized Intranasal
Midazolam in Children Undergoing Laceration Repair." J Emerg Med
53(3): 397-404.
168. Milesi, C., J. Baleine, et al. (2017). "Nasal
midazolam vs ketamine for neonatal intubation in the delivery room: a
randomised trial." Arch Dis Child Fetal Neonatal Ed.
169.
Miller, J., L. Ding, et al. (2017). "Sedation methods for transthoracic
echocardiography in children with Trisomy 21-a retrospective study."
Paediatr Anaesth 27(5):
531-539.
170.
Spalink, C. L., E. Barnes, et al. (2017). "Intranasal dexmedetomidine
for adrenergic crisis in familial dysautonomia." Clin Auton Res
27(4): 279-282.
173.
Liu, J., M. Du, et al. (2019). "Sedation effects of intranasal
dexmedetomidine combined with ketamine and risk factors for sedation
failure in young children during transthoracic echocardiography."
Paediatr Anaesth 29(1): 77-84.
174.
Messeha, M. M. and G. Z. El-Morsy (2018). "Comparison of Intranasal
Dexmedetomidine Compared to Midazolam as a Premedication in Pediatrics
with Congenital Heart Disease Undergoing Cardiac Catheterization."
Anesth Essays Res 12(1): 170-175.
175.
Milesi, C., J. Baleine, et al. (2018). "Nasal midazolam vs ketamine for
neonatal intubation in the delivery room: a randomised trial." Arch
Dis Child Fetal Neonatal Ed
103(3): F221-F226.
176. Olgun, G.
and M. H. Ali (2018). "Use of Intranasal Dexmedetomidine as a Solo
Sedative for MRI of Infants." Hosp Pediatr.
177.
Reynolds, J. and D. J. Sedillo (2018). "The Evolving Role of Intranasal
Dexmedetomidine for Pediatric Procedural Sedation." Hosp Pediatr.
178.
Ryan, P. M., A. J. Kienstra, et al. (2019). "Safety and effectiveness of
intranasal midazolam and fentanyl used in combination in the pediatric
emergency department." Am J Emerg Med
37(2): 237-240.
179.
Yang, F., Y. Liu, et al. (2019). "Analysis of 17 948 pediatric patients
undergoing procedural sedation with a combination of intranasal
dexmedetomidine and ketamine." Paediatr Anaesth
29(1): 85-91.
180.
Kunusoth, R., G. Tej, et al. (2019). "Comparative Analysis of
Intravenous Midazolam with Nasal Spray for Conscious Sedation in Minor
Oral and Maxillofacial Surgeries." J Pharm Bioallied Sci
11(Suppl 1): S42-S50.
181.
Sado-Filho, J., K. A. Viana, et al. (2019). "Randomized clinical trial
on the efficacy of intranasal or oral ketamine-midazolam combinations
compared to oral midazolam for outpatient pediatric sedation." PLoS
One 14(3): e0213074.
182.
Liu, S., Y. Wang, et al. (2019). "Safety and sedative effect of
intranasal182 dexmedetomidine in mandibular third molar surgery: a
systematic review and meta-analysis." Drug Des Devel Ther
13: 1301-1310.
183.
Oriby, M. E. (2019). "Comparison of Intranasal Dexmedetomidine and Oral
Ketamine Versus Intranasal Midazolam Premedication for Children
Undergoing Dental Rehabilitation." Anesth Pain Med
9(1): e85227.
184.
Sathyamoorthy, M., T. B. Hamilton, et al. (2019). "Pre-medication before
dental procedures: A randomized controlled study comparing intranasal
dexmedetomidine with oral midazolam." Acta Anaesthesiol Scand
63(9): 1162-1168.
185.
Syed, S., T. Hakim, et al. (2019). "To Evaluate the Efficiency of
Dexmedetomidine in Atomized Intranasal form for Sedation in Minor Oral
Surgical Procedures." Ann Maxillofac Surg
9(1): 89-95.
186.
Guthrie, A. M., R. A. Baum, et al. (2019). "Use of Intranasal Ketamine
in Pediatric Patients in the Emergency Department." Pediatr Emerg
Care.
187.
Malia, L., V. M. Laurich, et al. (2019). "Adverse events and
satisfaction with use of intranasal midazolam for emergency department
procedures in children." Am J Emerg Med
37(1): 85-88.
188.
Miguez, M. C., C. Ferrero, et al. (2019). "Retrospective Comparison of
Intranasal Fentanyl and Inhaled Nitrous Oxide to Intravenous Ketamine
and Midazolam for Painful Orthopedic Procedures in a Pediatric Emergency
Department." Pediatr Emerg Care.
189.
Williams, J. M., S. Schuman, et al. (2019). "Intranasal Fentanyl and
Midazolam for Procedural Analgesia and Anxiolysis in Pediatric Urgent
Care Centers." Pediatr Emerg Care.
190.
Khalil, W. and N. Raslan (2019). "The effectiveness of topical lidocaine
in relieving pain related to intranasal midazolam sedation: a
randomized, placebo-controlled clinical trial." Quintessence Int:
2-7.
191.
Alp, H., A. M. Elmaci, et al. (2019). "Comparison of intranasal
midazolam, intranasal ketamine, and oral chloral hydrate for conscious
sedation during paediatric echocardiography: results of a prospective
randomised study." Cardiol Young
29(9): 1189-1195.
192.
Li, B. L., V. M. Yuen, et al. (2019). "A Comparison of Intranasal
Dexmedetomidine and Dexmedetomidine Plus Buccal Midazolam for
Non-painful Procedural Sedation in Children with Autism." J Autism
Dev Disord 49(9): 3798-3806.
193.
Tenney, J. R., J. W. Miller, et al. (2019). "Intranasal Dexmedetomidine
for Sedation During Magnetoencephalography." J Clin Neurophysiol
36(5): 371-374.
194.
Trevisan, M., S. Romano, et al. (2019). "Intranasal dexmedetomidine and
intravenous ketamine for procedural sedation in a child with alpha-mannosidosis:
a magic bullet?" Ital J Pediatr
45(1): 119.
195.
Uusalo, P., S. Guillaume, et al. (2019). "Pharmacokinetics and Sedative
Effects of Intranasal Dexmedetomidine in Ambulatory Pediatric Patients."
Anesth Analg.
196.
Uusalo, P., M. Lehtinen, et al. (2019). "Premedication with intranasal
dexmedetomidine decreases barbiturate requirement in pediatric patients
sedated for magnetic resonance imaging: a retrospective study." BMC
Anesthesiol 19(1): 22.
197.
Gu, H. B., Y. A. Song, et al. (2019). "Median Effective Dose of
Intranasal Dexmedetomidine for Transthoracic Echocardiography in
Children with Kawasaki Disease Who Have a History of Repeated Sedation."
Med Sci Monit 25: 381-388.
198.
Liu, H., M. Sun, et al. (2019). "Determination of the 90% effective dose
of intranasal dexmedetomidine for sedation during electroencephalography
in children." Acta Anaesthesiol Scand
63(7): 847-852.
199.
Liu, J., M. Du, et al. (2019). "Sedation effects of intranasal
dexmedetomidine combined with ketamine and risk factors for sedation
failure in young children during transthoracic echocardiography."
Paediatr Anaesth 29(1):
77-84.
200.
Yang, F., S. Li, et al. (2019). "Fifty Percent Effective Dose of
Intranasal Dexmedetomidine Sedation for Transthoracic Echocardiography
in Children With Cyanotic and Acyanotic Congenital Heart Disease." J
Cardiothorac Vasc Anesth.
201.
Yang, F., Y. Liu, et al. (2019). "Analysis of 17 948 pediatric patients
undergoing procedural sedation with a combination of intranasal
dexmedetomidine and ketamine." Paediatr Anaesth
29(1): 85-91.
202.
Chen, C., M. You, et al. (2019). "Study of Feasibility and Safety of
Higher-Dose Dexmedetomidine in Special Outpatient Examination of
Pediatric Ophthalmology." J Ophthalmol
2019: 2560453.
203.
Bregstein, J. S., A. M. Wagh, et al. (2019). "Intranasal Lorazepam for
Treatment of Severe Agitation in a Pediatric Behavioral Health Patient
in the Emergency Department." Ann Emerg Med.
204.
Li, B. L., V. M. Yuen, et al. (2019). "A Comparison of Intranasal
Dexmedetomidine and Dexmedetomidine Plus Buccal Midazolam for
Non-painful Procedural Sedation in Children with Autism." J Autism
Dev Disord 49(9): 3798-3806.
205.
Bi, Y., Y. Ma, et al. (2019). "Efficacy of premedication with intranasal
dexmedetomidine for removal of inhaled foreign bodies in children by
flexible fiberoptic bronchoscopy: a randomized, double-blind,
placebo-controlled clinical trial." BMC Anesthesiol
19(1): 219.
206.
Lewis, J. and C. R. Bailey (2019). "Intranasal dexmedetomidine for
sedation in children; a review." J Perioper Pract:
1750458919854885.
207.
Mondardini, M. C., A. Amigoni, et al. (2019). "Intranasal
dexmedetomidine in pediatrics: update of current knowledge." Minerva
Anestesiol 85(12): 1334-1345.
208.
Uusalo, P., H. Jatinvuori, et al. (2019). "Intranasal Low-Dose
Dexmedetomidine Reduces Postoperative Opioid Requirement in Patients
Undergoing Hip Arthroplasty Under General Anesthesia." J Arthroplasty
34(4): 686-692 e682.
209.
Wang, C. Y., H. Ihmsen, et al. (2019). "Pharmacokinetics of Intranasally
Administered Dexmedetomidine in Chinese Children." Front Pharmacol
10: 756.
210.
Ku, L. C., C. Simmons, et al. (2019). "Intranasal midazolam and fentanyl
for procedural sedation and analgesia in infants in the neonatal
intensive care unit." J Neonatal Perinatal Med
12(2): 143-148.
218. Barends, C.R.M., et al., Intranasal dexmedetomidine in elderly subjects with or without beta blockade: a randomised double-blind single-ascending-dose cohort study. Br J Anaesth, 2020.
219. Chen, H., et al., Intranasal dexmedetomidine is an effective sedative agent for electroencephalography in children. BMC Anesthesiol, 2020. 20(1): p. 61.
220. Yao, Y., et al., Intranasal dexmedetomidine versus oral midazolam premedication to prevent emergence delirium in children undergoing strabismus surgery: A randomised controlled trial. Eur J Anaesthesiol, 2020. 37(12): p. 1143-1149.
221.
226. Wang, F. H., J. Zhang, et al. (2020). "[Sedative effect of intranasal
midazolam in neonates undergoing magnetic resonance imaging: a
prospective single-blind randomized controlled study]." Zhongguo Dang
Dai Er Ke Za Zhi 22(5):
441-445.