 Therapeutic
Intranasal Drug Delivery
Therapeutic
Intranasal Drug DeliveryAnatomy and Physiology of the nose: Key points relating to nasal drug delivery
Table of Contents
Nasal Cavity function (Click here)
Nasal mucosal absorption of medications into blood stream (Click here)
Nose-brain pathway - absorption of medications into brain and CSF (Click here)
Peer Reviewed articles (Click here)
Nasal Cavity function: Olfaction, filtration, heating and humidification:
The nose has two primary functions. The first is
olfaction – the sense of smell. However, the second function is of
primary interest to this discussion – filtration, heating and
humidification of the inhaled air.
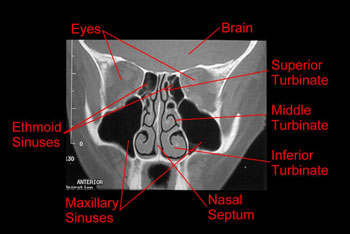 To
accomplish the second task, the nasal cavity contains a convoluted set
of passageways called the turbinates on the lateral wall of each nasal
cavity (see cross-sectional CT scan of turbinates to right). These
turbinates interrupt the flow of air into the nasal passage, forcing it
through narrow passages that are covered with moist nasal respiratory
mucosa. The total surface area available in the nasal mucosa is
estimated to be about 180 cm2, of which 10 cm2 is
olfactory mucosa and 170 cm2 is the richly vascularized
respiratory mucosa.
To
accomplish the second task, the nasal cavity contains a convoluted set
of passageways called the turbinates on the lateral wall of each nasal
cavity (see cross-sectional CT scan of turbinates to right). These
turbinates interrupt the flow of air into the nasal passage, forcing it
through narrow passages that are covered with moist nasal respiratory
mucosa. The total surface area available in the nasal mucosa is
estimated to be about 180 cm2, of which 10 cm2 is
olfactory mucosa and 170 cm2 is the richly vascularized
respiratory mucosa.
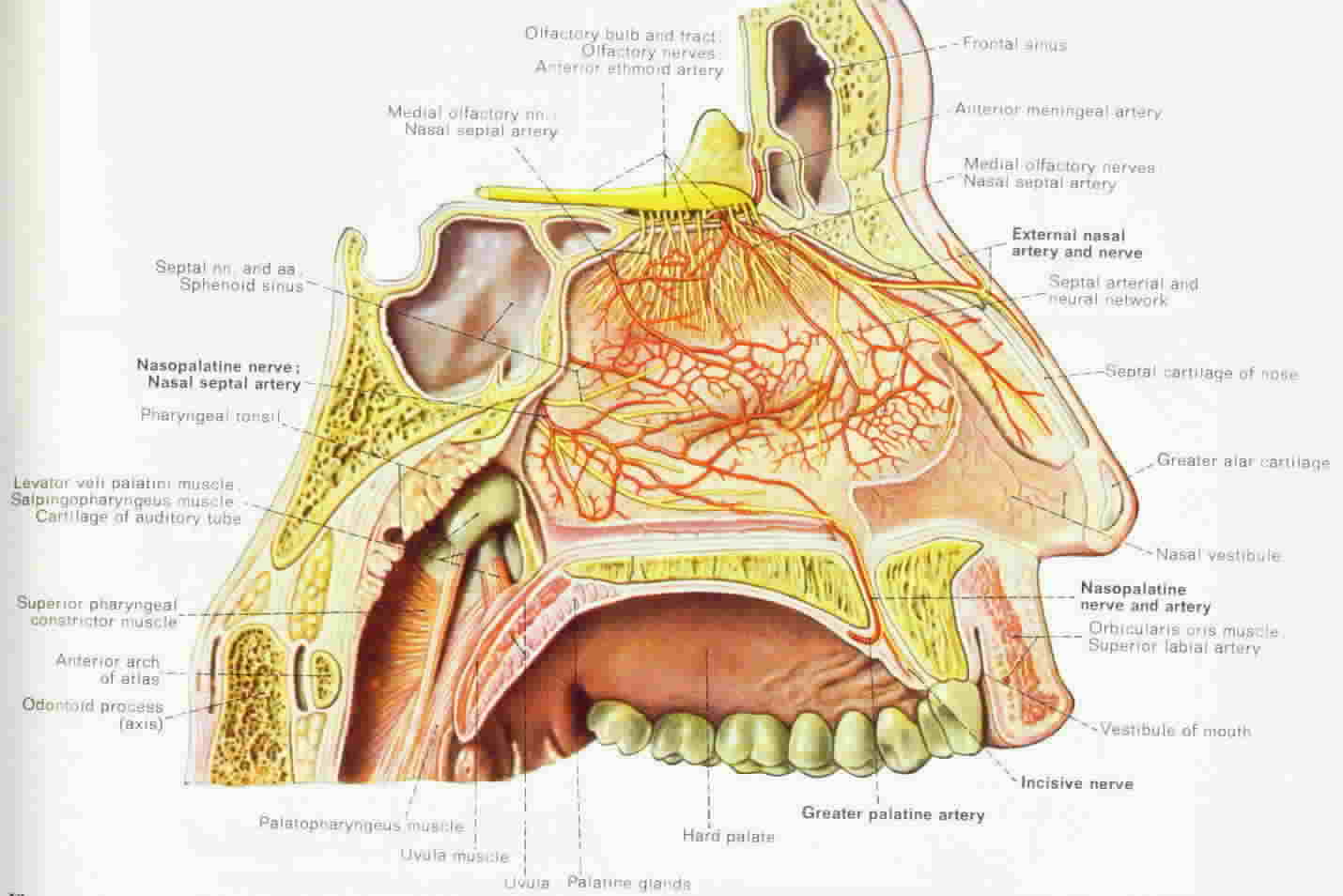 During
the passage across this broad mucosal surface, the air is warmed and
humidified by a rich vascular capillary bed that is directly beneath the
surface see diagram to left). These capillaries are specifically
designed for rapid passage of fluids through the vascular wall and out
into the dry air.[1-3] The amount of blood flow to this area is
considerable – it is higher per unit of tissue than the blood flow to
the brain, liver or muscle.[2-4]
During
the passage across this broad mucosal surface, the air is warmed and
humidified by a rich vascular capillary bed that is directly beneath the
surface see diagram to left). These capillaries are specifically
designed for rapid passage of fluids through the vascular wall and out
into the dry air.[1-3] The amount of blood flow to this area is
considerable – it is higher per unit of tissue than the blood flow to
the brain, liver or muscle.[2-4]
Nasal mucosal absorption of medications directly into the blood stream:
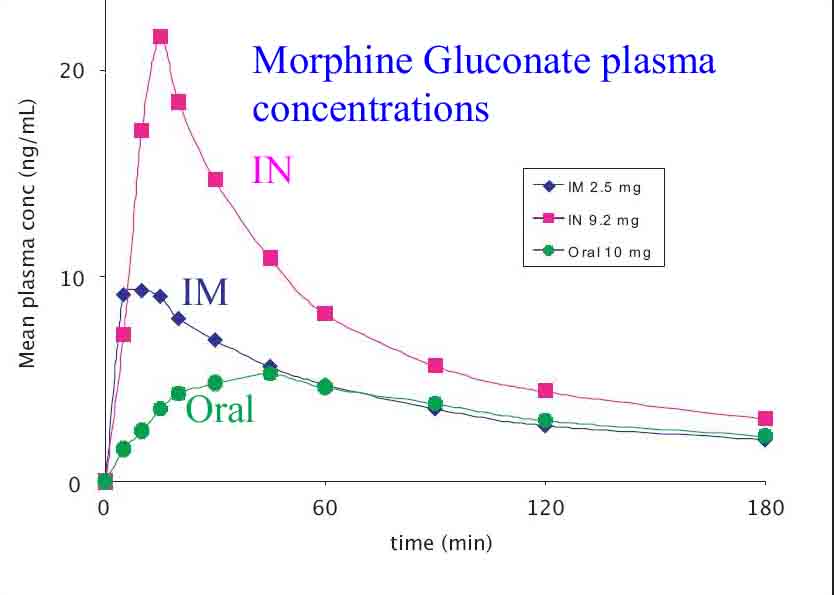 This
large mucosal surface covered with a rich vascular bed of highly
permeable capillaries creates an opportunity for intranasal medication
delivery. Not only will fluids cross the capillary bed into the air
stream to humidify the air, but fluids delivered in the air stream onto
the mucosa will also cross the capillary bed into the blood stream.[1-3]
For this reason, when medications of proper concentration and molecular
character are delivered onto the nasal mucosa, they are rapidly
transported into the capillary bed and delivered to the patient’s
circulation. (See diagram comparing nasal morphine plasma concentrations
to thos
This
large mucosal surface covered with a rich vascular bed of highly
permeable capillaries creates an opportunity for intranasal medication
delivery. Not only will fluids cross the capillary bed into the air
stream to humidify the air, but fluids delivered in the air stream onto
the mucosa will also cross the capillary bed into the blood stream.[1-3]
For this reason, when medications of proper concentration and molecular
character are delivered onto the nasal mucosa, they are rapidly
transported into the capillary bed and delivered to the patient’s
circulation. (See diagram comparing nasal morphine plasma concentrations
to thos
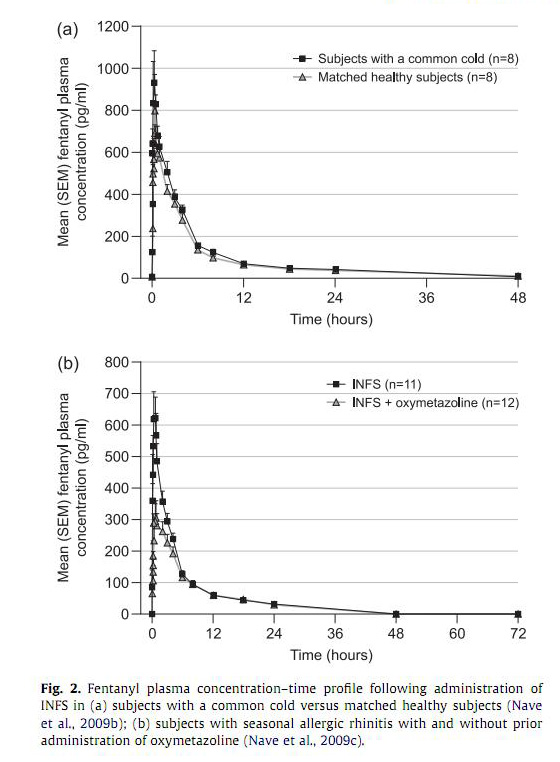
There are some patient factors that would theoretically limit nasal absorption. A significant amount of mucous or blood on the nasal mucosa may prevent drug absorption or result in rapid washing away of the medication. Prior use of vasoconstrictors such as oxymetazoline, phenylephrine or cocaine might also limit absorption. Investigators have confirmed that vasoconstrictors will reduce (but not eliminate) drug absorption while a mild URI will have little or no effect (see diagram).[10]
Nose-brain pathway – nasal mucosal absorption of medications directly into the cerebral spinal fluid and brain:
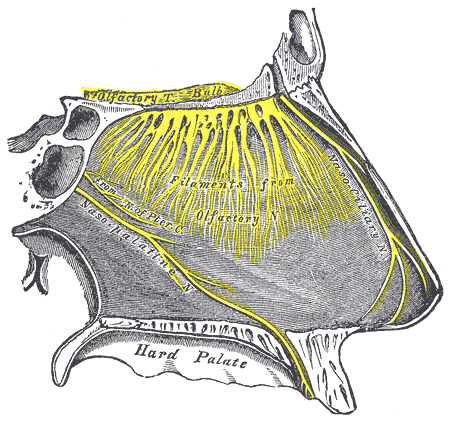 If
the nasally administered medication contacts the olfactory mucosa, there
is good evidence that suggests molecule transport can occur directly
across this tissue and into the cerebral spinal fluid.[5-8] The
olfactory mucosa is located in the upper nasal cavity, just below the
cribriform plate of the skull. It contains olfactory cells which
traverse the cribriform plate and extend up into the cranial cavity.
When medication molecules come in contact with this specialized mucosa
they are rapidly transported directly into the brain, skipping the
blood-brain barrier, and achieving very rapid cerebrospinal fluid levels
(often faster than if the drug is given intravenously).
If
the nasally administered medication contacts the olfactory mucosa, there
is good evidence that suggests molecule transport can occur directly
across this tissue and into the cerebral spinal fluid.[5-8] The
olfactory mucosa is located in the upper nasal cavity, just below the
cribriform plate of the skull. It contains olfactory cells which
traverse the cribriform plate and extend up into the cranial cavity.
When medication molecules come in contact with this specialized mucosa
they are rapidly transported directly into the brain, skipping the
blood-brain barrier, and achieving very rapid cerebrospinal fluid levels
(often faster than if the drug is given intravenously).
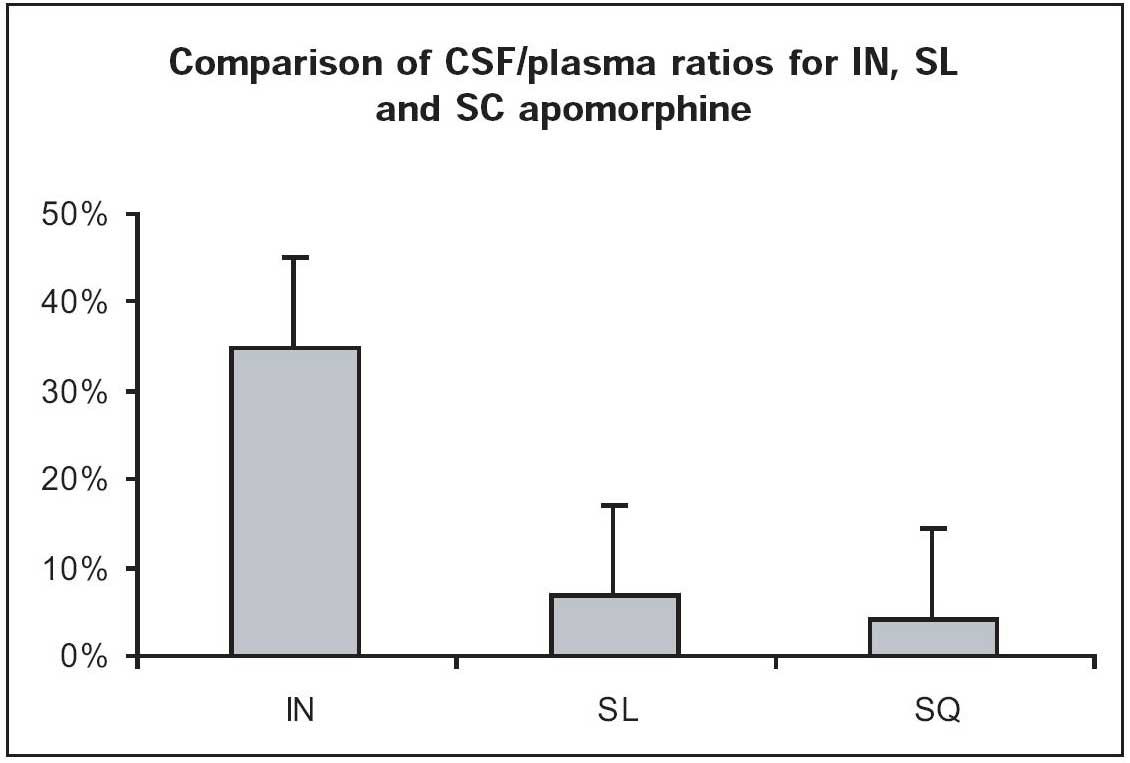 This
concept of transfer of molecules from the nose to the brain is referred
to as the nose-brain pathway and has implications when centrally acting
medications such as sedatives, anti-seizure drugs and opiates are
delivered nasally. Multiple authors demonstrate that the nose-brain
pathway leads to nearly immediate delivery of some nasal medications to
the cerebral spinal fluid, by-passing the blood brain barrier.[5-9,11,
12]
This
concept of transfer of molecules from the nose to the brain is referred
to as the nose-brain pathway and has implications when centrally acting
medications such as sedatives, anti-seizure drugs and opiates are
delivered nasally. Multiple authors demonstrate that the nose-brain
pathway leads to nearly immediate delivery of some nasal medications to
the cerebral spinal fluid, by-passing the blood brain barrier.[5-9,11,
12]
Literature related to Nose brain pathway:
Talegaonkar, IN delivery and BBB, Indian J Pharm 2004.pdf
Westin, Olfactory transfer of analgesic drugs after nasal administration, Thesis paper 2007
Summary:
In summary, the nasal mucosa consists of a highly vascularized surface that easily absorbs many medications directly into the venous circulation. This medication is then transported to the heart and pumped out to the body where it can have its therapeutic effect. Because the absorptive surface is not the intestinal mucosa, the drug never enters the portal circulation and is not subjected to hepatic metabolism – thereby leading to far higher drug levels than oral or rectal medications. In addition, the nose brain pathway across the olfactory mucosal transports some of the nasally delivered medication directly into the CSF and brain – leading to early effects of centrally acting medications.
Education:
Peer Reviewed Articles:
- Hanson, IN drugs for neurodegenerative disorders, Policy Holder Advocate.pdf
- Pires, Intranasal drug delivery - How why what for -extensive review, J Pharm Pharmaceut Sci 2009
- Talegaonkar, Intranasal delivery - An approach to bypass the blood brain barrier, I J Pharm 2004.pdf
- Ying, Nose-brain path and neurologic diseases, Future medicine.pdf
-
Bibliography (Click here for abstracts):
1. Hussain, A.A., Mechanism of nasal absorption of drugs. Prog Clin Biol Res, 1989. 292: p. 261-272.
2. Dale, O., R. Hjortkjaer, and E.D. Kharasch, Nasal administration of opioids for pain management in adults. Acta Anaesthesiol Scand, 2002. 46(7): p. 759-70.
3. Chien, Y.W., K.S.E. Su, and S.F. Chang, Chapter 1: Anatomy and Physiology of the Nose. Nasal Systemic Drug Delivery, 1989. Dekker, New York: p. 1-26.
4. Mygind, N. and S. Vesterhauge, Aerosol distribution in the nose. Rhinology, 1978. 16(2): p. 79-88.
5. Henry, R.J., et al., A pharmacokinetic study of midazolam in dogs: nasal drop vs. atomizer administration. Pediatr Dent, 1998. 20(5): p. 321-6.
6. Sakane, T., et al., Transport of cephalexin to the cerebrospinal fluid directly from the nasal cavity. J Pharm Pharmacol, 1991. 43(6): p. 449-51.
7. Banks, W.A., M.J. During, and M.L. Niehoff, Brain uptake of the glucagon-like peptide-1 antagonist exendin(9-39) after intranasal administration. J Pharmacol Exp Ther, 2004. 309(2): p. 469-75.
8. Westin, et al., Direct nose-to-brain transfer of morphine after nasal administration to rats. Pharm Res, 2006. 23(3): p. 565-72.
9.
Cros,
C. D., I. Toth, et al. (2014). "Delivery of a lactose derivative of
endomorphin 1 to the brain via the olfactory epithelial pathway."
Bioorg Med Chem Lett 24(5):
1373-1375.
10. Dale, O., Intranasal administration of opioids/fentanyl - Physiological and pharmacological aspects. European Journal of Pain Supplements, 2010. www.europeanjournalpain.com: p. volume and pages pending.
11. Md, S., et al., Optimised nanoformulation of bromocriptine for direct nose-to-brain delivery: biodistribution, pharmacokinetic and dopamine estimation by ultra-HPLC/mass spectrometry method. Expert Opin Drug Deliv, 2014. 11(6): p. 827-42.
12.
Iwasaki, S., S. Yamamoto, et al. (2019). "Direct Drug Delivery of
Low-Permeable Compounds to the Central Nervous System Via Intranasal
Administration in Rats and Monkeys." Pharm Res
36(5): 76.